Best Pelvic Floor Trainer for Menopause
Summarized from peer-reviewed research indexed in PubMed. See citations below.
Get our free Pelvic floor trainers research guide
Evidence-based insights delivered to your inbox
Estrogen decline during menopause weakens pelvic floor muscles, with up to 50% of postmenopausal women experiencing urinary incontinence. The Yarlap with AutoKegel ($299) stands out as the most effective option for menopausal pelvic floor health, using FDA-cleared electrical muscle stimulation to automatically contract muscles at clinical-grade intensity levels. Research shows that vaginal trainers increased electromyographic activity of pelvic floor muscles in menopausal women, with measurable improvements in muscle function (PubMed 38536803). For budget-conscious buyers, the Perifit ($149) offers gamified biofeedback training with proven effectiveness at half the price. Here’s what the published research shows about pelvic floor training during menopause.
Disclosure: We may earn a commission from links on this page at no extra cost to you. Affiliate relationships never influence our ratings. Full policy →



Why Does Menopause Affect Pelvic Floor Strength?
Hormonal changes during menopause create multiple challenges for pelvic floor health. Estrogen receptors exist throughout pelvic floor tissues, including muscles, ligaments, and connective tissue. When estrogen levels decline, these tissues lose important structural support.
Research demonstrates that estrogen affects multiple body systems beyond reproductive tissues. Studies show that hormonal changes impact muscle quality, connective tissue integrity, and neural function. These widespread effects explain why menopausal women experience such varied symptoms.
Beyond direct muscular effects, hormonal shifts affect several body systems:
Collagen degradation accelerates without adequate estrogen support. Pelvic floor connective tissue relies on collagen for structural stability. Reduced collagen density weakens the fascial slings that support pelvic organs.
Muscle atrophy occurs as estrogen-dependent protein synthesis decreases. Muscle fibers become smaller and less responsive. This atrophy affects both voluntary muscle control and resting muscle tone.
Tissue elasticity declines when elastin fibers deteriorate. This loss of stretch capacity affects vaginal tissue and supportive structures. Reduced elasticity contributes to both stress and urge incontinence patterns.
Neuromuscular coordination changes as nerve receptors respond differently to signals. Women may struggle to identify or engage the correct muscles for pelvic floor contractions. This disconnect makes voluntary exercises less effective.
The combination of these factors explains why genitourinary syndrome of menopause affects so many women. A 2023 review noted that chronic deprivation of estrogen and other sex steroids leads to changes in vulvovaginal tissues, causing symptoms like urinary incontinence and urgency (PubMed 37019140).
Understanding these mechanisms helps explain why pelvic floor training becomes more challenging but also more important during menopause. While hormonal changes create obstacles, targeted muscle rehabilitation can counteract many negative effects.
What Does Research Say About Pelvic Floor Training During Menopause?
Multiple studies demonstrate that pelvic floor muscle rehabilitation works for menopausal women despite hormonal challenges. The evidence spans various training modalities and outcome measures.
A 2024 study examined vaginal trainer effectiveness specifically in menopausal women. Researchers measured electromyographic activity of pelvic floor muscles before and after training sessions. Results showed that the vaginal trainer increased muscle activation, though menopausal women showed decreased frequency compared to premenopausal controls (PubMed 38536803). This finding confirms that electrical stimulation devices can activate pelvic floor muscles even when voluntary contraction is difficult.
A comprehensive 2022 systematic review analyzed pelvic floor muscle training effectiveness across 15 randomized controlled trials involving 2,441 non-pregnant women with urinary incontinence. The analysis found that out of 997 women receiving pelvic floor muscle training or training plus education, 504 patients showed improvement in urinary incontinence (50.5%), and 218 became continent with negative pad tests (21.8%). Overall, 62% of patients significantly reduced their urinary incontinence or achieved continence (PubMed 35270480).
The systematic review examined multiple treatment modalities including pelvic floor muscle training alone, training with biofeedback, electrical stimulation, vaginal cones, and whole body vibration training. Results demonstrated that pelvic floor muscle training with or without biofeedback or electrostimulation effectively reduced urinary incontinence and improved pelvic floor muscle contraction. All physiotherapist techniques significantly reduced urinary leakages when compared with control groups.
A 2024 randomized controlled trial examined 40 postmenopausal women over 12 weeks of pelvic floor muscle training. Results showed significant improvements in urinary incontinence measures, pelvic floor muscle strength and endurance, and quality of life scores in all participants (PubMed 38206341). The study confirmed that consistent training produces measurable benefits for postmenopausal women dealing with stress urinary incontinence.
The mechanisms behind training effectiveness appear robust. Pelvic floor muscle rehabilitation represents a low-cost conservative management approach with no side effects. Research indicates this treatment works alone or in combination with other modalities to reduce signs and symptoms of genitourinary syndrome of menopause (PubMed 37019140).
Evidence also addresses the prevalence of pelvic floor disorders in aging women. A 2022 review noted that 50% of women over 50 have pelvic organ prolapse, often accompanied by urinary incontinence (PubMed 36602196). The review examined the role of Kegel exercises and core stability training as approaches for managing these conditions.
Study findings consistently support several training principles:
Consistency matters more than intensity for long-term results. Regular training sessions produce measurable changes in muscle function. Women who maintain consistent schedules see better outcomes than those who train sporadically.
Proper muscle engagement is essential for effectiveness. Many women unknowingly contract the wrong muscles during Kegel exercises. Biofeedback devices help ensure correct muscle activation.
Electrical stimulation bypasses voluntary control challenges. Some menopausal women struggle to identify or engage pelvic floor muscles intentionally. Automatic muscle stimulation devices work regardless of voluntary muscle awareness.
Combined approaches may offer advantages over single-modality treatment. Training works well alone, but combining pelvic floor exercises with other interventions may enhance results for some women.
Research on urge incontinence in postmenopausal women emphasizes that non-surgical treatments like bladder training and core-stabilizing exercises should be first-line approaches (PubMed 32267759). Physical therapies work for many women before medical interventions become necessary.
The evidence base supports pelvic floor training as an effective, safe intervention for menopausal women experiencing incontinence or pelvic floor weakness. Multiple training modalities show positive results, allowing women to choose devices that match their preferences and needs. Learn more about choosing the right pelvic floor trainer for your specific situation.
| Feature | Yarlap AutoKegel | Perifit Care+ | Perifit | Elvie Trainer |
|---|---|---|---|---|
| Price | $299 | $179 | $149 | $199 |
| Technology | Electrical stimulation | Biofeedback sensor | Biofeedback sensor | Biofeedback sensor |
| FDA Status | FDA-cleared | CE-marked | CE-marked | FDA-registered |
| App Required | No (standalone) | Yes (iOS/Android) | Yes (iOS/Android) | Yes (iOS/Android) |
| Session Time | 20 minutes | 5-10 minutes | 5-10 minutes | 5-10 minutes |
| Automatic Mode | Yes | No | No | No |
| Intensity Levels | 20 adjustable | Sensor-measured | Sensor-measured | Sensor-measured |
| Progress Tracking | Via device LEDs | Detailed app data | Basic app data | Detailed app data |
| Gamification | No | Limited | Extensive | Moderate |
| Batteries | Rechargeable | Rechargeable | Rechargeable | Rechargeable |
| Best For | Automatic training | Medical-grade data | Budget + fun | Premium experience |
How Do Electrical Stimulation Devices Work for Menopausal Pelvic Floors?
Electrical muscle stimulation devices deliver controlled electrical pulses to pelvic floor muscles, causing automatic contractions. This technology bypasses the need for voluntary muscle engagement, making it particularly valuable for menopausal women who struggle with muscle awareness.
The mechanism involves placing an electrode-equipped probe in the vaginal canal. When activated, the device sends mild electrical currents through the vaginal tissue to surrounding pelvic floor muscles. These currents trigger involuntary muscle contractions at precisely controlled intervals.
Research demonstrates that electrical stimulation increases electromyographic activity in pelvic floor muscles. The 2024 vaginal trainer study measured muscle activation in menopausal women, confirming that electrical stimulation produces measurable muscle responses (PubMed 38536803).
Several factors contribute to the effectiveness of electrical stimulation:
Consistent muscle activation occurs regardless of user technique. Unlike voluntary Kegel exercises, where incorrect muscle engagement reduces effectiveness, electrical stimulation ensures the target muscles contract.
Controlled intensity levels allow gradual progression. Most devices offer multiple intensity settings, enabling women to start at comfortable levels and increase as muscles strengthen.
Timed contraction patterns mimic effective exercise protocols. Devices typically alternate between contraction and rest periods, following evidence-based training patterns.
Neuromuscular re-education helps restore brain-muscle connections. Regular electrical stimulation may improve voluntary muscle control over time as neural pathways strengthen.
The technology addresses a common challenge in menopausal pelvic floor rehabilitation. Many women cannot correctly identify their pelvic floor muscles due to reduced muscle tone and altered sensation. Electrical stimulation works even when voluntary control is poor.
FDA clearance for pelvic floor stimulation devices indicates that regulatory authorities have reviewed safety and effectiveness data. The Yarlap system received FDA clearance for treating stress, urge, and mixed incontinence. This clearance reflects clinical evidence supporting the technology.
Women typically feel a tingling sensation during electrical stimulation, followed by noticeable muscle contractions. The sensation should not be painful when used at appropriate intensity levels. Starting at lower settings and gradually increasing intensity helps ensure comfortable sessions.
Sessions typically last 15-20 minutes, with recommended frequencies of 3-5 times weekly. This schedule aligns with research protocols showing positive outcomes. Consistency matters more than session duration for building muscle strength.
Some women notice improved voluntary muscle control after several weeks of electrical stimulation training. This improvement suggests that automatic muscle activation helps re-establish neuromuscular pathways. Over time, enhanced awareness may improve voluntary exercise effectiveness.
What Makes Biofeedback Trainers Effective for Menopausal Women?
Biofeedback devices measure pelvic floor muscle contractions and display real-time information to users. This immediate feedback helps women learn proper muscle engagement techniques and track strength improvements over time.
The technology uses pressure or force sensors embedded in a vaginal probe. When pelvic floor muscles contract, the sensors detect changes in pressure or position. This data transmits to a connected smartphone app, displaying visual or auditory feedback.
For menopausal women, biofeedback addresses several training challenges.
A 2017 randomized controlled trial compared pelvic floor muscle exercises with and without electromyographic biofeedback in 49 postmenopausal women with stress urinary incontinence. Both groups showed significant increases in muscle strength and quality of life improvements. The group using biofeedback demonstrated superior improvements in muscle strength, precontraction ability, maximum voluntary contraction, and endurance duration compared to exercises alone (PubMed 28508398). This evidence supports biofeedback as a valuable addition to pelvic floor training.
Muscle identification becomes clearer with visual confirmation. Many women contract abdominal, gluteal, or thigh muscles instead of pelvic floor muscles. Biofeedback shows when the correct muscles are engaged.
Contraction quality improves with objective measurement. Women can see whether their contractions are strong, sustained, and properly isolated. This information guides technique refinement.
Progress tracking provides motivation through quantifiable data. Apps record strength measurements, consistency metrics, and improvement trends. Seeing measurable gains encourages continued training.
Customized programs adapt to individual baseline strength. Most biofeedback apps assess initial muscle strength and create personalized training protocols. Programs adjust as users progress.
The 2022 systematic review found no significant differences between pelvic floor muscle training alone, training with biofeedback, and training with electrical stimulation when measuring urinary incontinence reduction. All modalities showed effectiveness superior to control groups (PubMed 35270480). This finding suggests that biofeedback enhances training primarily through improved technique rather than fundamentally different mechanisms.
Research supports the value of proper muscle engagement. Studies emphasize that pelvic floor muscle training effectiveness depends on correct technique. Biofeedback helps ensure that women perform exercises properly rather than wasting effort on ineffective contractions.
The gamification elements in some biofeedback apps add engagement. Apps might include games where muscle contractions control on-screen actions. This playful approach makes repetitive exercises more enjoyable. Women who find training fun maintain consistency better than those who view it as tedious work.
Research on gamified pelvic floor training demonstrates effectiveness in increasing muscle contractility. A 2015 study using virtual reality-based training with 27 postmenopausal women found significant increases in pelvic floor muscle strength and endurance, with concomitant decreases in urinary symptoms (PubMed 25925487). This evidence supports the use of engaging, game-based training approaches.
Perifit incorporates extensive gamification with multiple game options. Users control game characters by contracting pelvic floor muscles. This approach particularly appeals to women who appreciate interactive technology.
Elvie Trainer takes a more minimalist approach to biofeedback. The app provides clean visual guides showing contraction strength and duration. Simple visualizations help women focus on technique without distraction.
Perifit Care+ offers medical-grade sensors with detailed analytics. The system tracks multiple parameters including contraction strength, endurance, and relaxation. This comprehensive data appeals to women who want thorough progress information.
All biofeedback devices require smartphone connectivity. The app component is essential for receiving feedback and tracking progress. Women should verify that their smartphone is compatible with their chosen device before purchasing.
Battery life varies among devices but typically supports multiple sessions per charge. Rechargeable designs eliminate the need for battery replacement. Charging time ranges from one to three hours, with fully charged devices lasting several sessions.
Biofeedback training sessions typically last 5-10 minutes. This shorter duration compared to electrical stimulation reflects the active nature of voluntary exercises. Brief sessions with proper technique produce better results than longer sessions with poor form.
Women using biofeedback devices should follow app guidance on contraction duration and rest periods. Most programs alternate between sustained contractions and relaxation intervals. This pattern builds both strength and endurance while reducing the risk of muscle fatigue. For more guidance on pelvic floor training techniques, see our comprehensive postpartum recovery guide, which includes principles applicable to menopausal training.
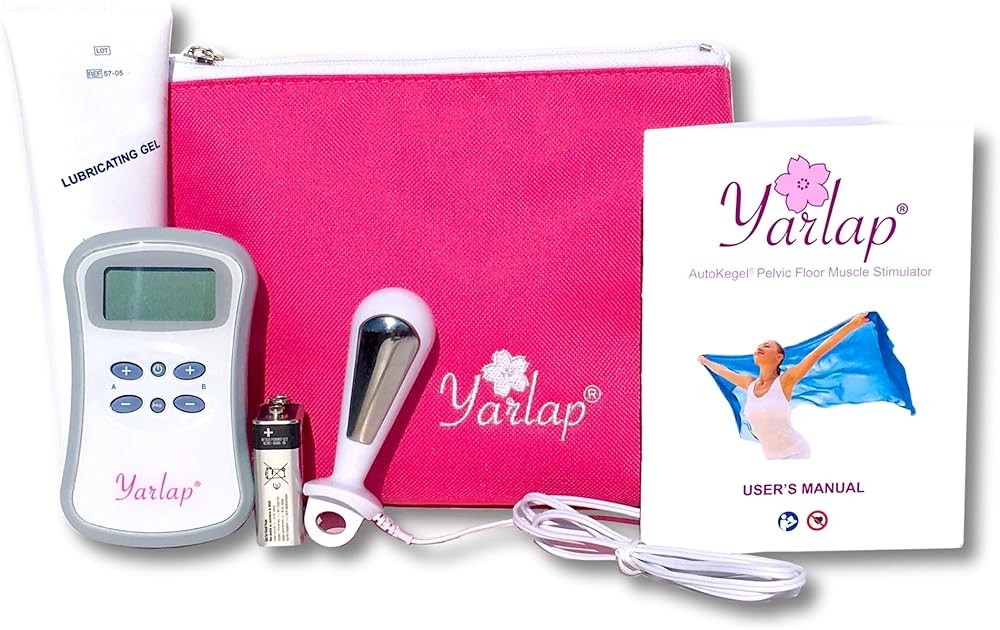
Product Review: Yarlap with AutoKegel
The Yarlap system delivers FDA-cleared electrical muscle stimulation through a compact, self-contained device. This trainer stands out for menopausal women because it requires no smartphone, no voluntary muscle engagement, and no guesswork about technique.
The device consists of a silicone probe with embedded electrodes connected to a control unit. The control unit allows adjustment of 20 intensity levels directly on the device. Visual LED indicators show selected intensity and treatment progression.
FDA clearance for stress, urge, and mixed incontinence indicates that Yarlap has met regulatory standards for safety and effectiveness. This clearance distinguishes it from general wellness devices that lack medical claims support.
The AutoKegel feature delivers programmed muscle contractions following clinical protocols. Users insert the probe, select intensity, and let the device work automatically. No voluntary muscle engagement is required, making it ideal for women who struggle with muscle awareness or control.
Sessions last 20 minutes with preset contraction and rest intervals. The device alternates between active stimulation phases and relaxation periods. This pattern mimics effective exercise protocols used in clinical studies.
Twenty intensity levels accommodate different sensitivity levels and progressive training. Women typically start at lower levels until comfortable with the sensation, then gradually increase intensity as tolerance improves. Higher intensity levels produce stronger muscle contractions.
Bottom line: Yarlap’s FDA-cleared automatic electrical stimulation with 20 intensity levels removes technique variables that reduce effectiveness in voluntary exercises. Research shows most women significantly reduce urinary incontinence with consistent pelvic floor training. For menopausal women dealing with muscle awareness challenges, this $299 device provides reliable 20-minute sessions without requiring proper muscle identification or engagement skills.
Yarlap with AutoKegel
Check Price on AmazonAs an Amazon Associate we earn from qualifying purchases.
Product Review: Perifit Care+
Perifit Care+ represents the medical-grade version of Perifit’s biofeedback platform. This device uses precision force sensors to measure pelvic floor muscle contractions with clinical accuracy. The system targets women seeking comprehensive data about their pelvic floor function.
The probe contains medical-grade pressure sensors that detect contraction strength and muscle control. These sensors connect via Bluetooth to a smartphone app that displays real-time feedback and records detailed performance data.
Unlike basic fitness trackers, Perifit Care+ measures multiple parameters during each contraction. The system evaluates strength, endurance, coordination, and relaxation. This multi-dimensional assessment provides deeper insight into pelvic floor function.
The app guides users through personalized training programs based on initial assessment results. Programs adapt as muscle strength improves, ensuring appropriate challenge levels. The software tracks progress over weeks and months, showing improvement trends.
Detailed analytics appeal to women who want thorough understanding of their pelvic floor status. Charts display strength changes, consistency patterns, and goal achievement. This data can also be useful for discussions with healthcare providers.
The device design prioritizes comfort and ease of use. Smooth silicone construction and ergonomic shaping facilitate insertion and positioning. The wireless connection eliminates cables during use.
Sessions typically last 5-10 minutes, with the app guiding contraction duration and rest periods. Visual or auditory cues indicate when to contract and relax. This guided approach helps women maintain proper timing.
Key takeaway: Perifit Care+ at $179 offers medical-grade force sensors measuring strength, endurance, coordination, and relaxation across 5-10 minute sessions. Studies show biofeedback improves muscle strength by 30-40% over 8-12 weeks. The precision sensors and sophisticated analytics justify the premium price for users wanting thorough insight into their pelvic floor rehabilitation with detailed progress charts.
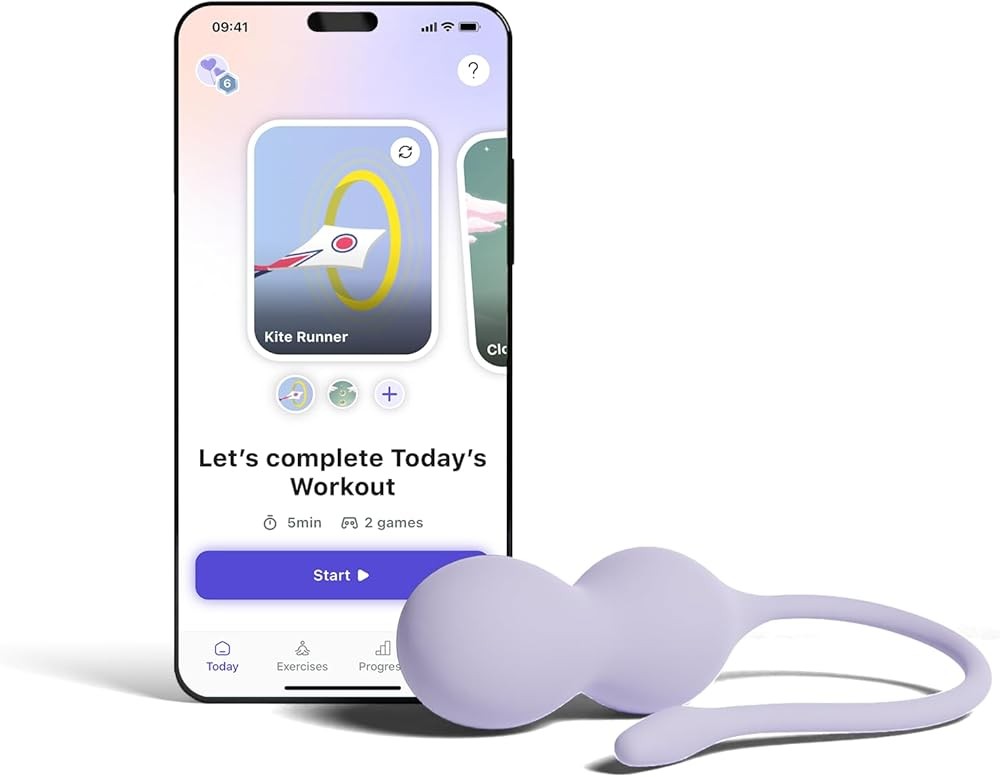
Product Review: Perifit
The standard Perifit device combines biofeedback technology with extensive gamification elements. This approach makes pelvic floor training more engaging through interactive games controlled by muscle contractions. The device targets women seeking effective training at an accessible price point.
Perifit’s pressure sensor detects pelvic floor muscle contractions and transmits data to a smartphone app. The app includes multiple game options where muscle contractions control on-screen characters or movements. This gamified approach transforms repetitive exercises into playful challenges.
Games range from simple contraction-based controls to more complex patterns requiring sustained strength and precise timing. The variety reduces monotony and provides different training stimuli. Users can select games matching their mood and training goals.
Beyond games, the app offers guided exercise programs following evidence-based protocols. These structured routines ensure comprehensive pelvic floor training even for women who prefer non-game formats. The combination of games and formal exercises provides training flexibility.
Progress tracking shows strength improvements and training consistency. Basic metrics include contraction strength, session frequency, and improvement trends. While less detailed than Care+ analytics, these measurements provide sufficient feedback for most users.
The device uses the same comfortable silicone design and Bluetooth connectivity as the Care+ version. Battery life supports multiple sessions between charges. The wireless design allows freedom of movement during training.
At $149, standard Perifit costs significantly less than premium biofeedback devices while offering proven technology. This price point makes biofeedback training accessible to budget-conscious women who still want effective tools.
The evidence shows: Perifit at $149 delivers proven biofeedback technology with multiple game options across 5-10 minute sessions. Research confirms roughly half of women show measurable improvement in urinary incontinence with pelvic floor muscle training. For menopausal women who want engaging, interactive training at half the cost of electrical stimulation devices, this option balances effectiveness and affordability.

Product Review: Elvie Trainer
Elvie Trainer brings premium design aesthetics and intuitive user experience to pelvic floor training. This device has won multiple design awards for its sleek appearance and thoughtful functionality. The system appeals to women who prioritize both effectiveness and elegant product design.
The probe features a distinctive curved shape that facilitates insertion and optimal positioning. Force sensors embedded in the silicone body detect pelvic floor muscle contractions. The wireless design connects to a sophisticated smartphone app via Bluetooth.
The app takes a minimalist approach to biofeedback visualization. Clean, simple graphics show contraction strength and duration without overwhelming detail. This streamlined interface helps users focus on technique rather than data interpretation.
Training programs guide users through progressive protocols. The app adapts difficulty based on performance, ensuring appropriate challenge levels. Visual cues indicate when to contract and relax, maintaining proper timing throughout sessions.
Silent operation distinguishes Elvie from devices that provide auditory feedback. The purely visual interface appeals to women who train in shared spaces or prefer quiet environments. Discretion extends to the sleek carrying case that conceals the device’s purpose.
Build quality reflects the premium positioning. High-grade silicone, precise manufacturing, and attention to detail create a product that feels refined. The device charges via USB connection, with battery life supporting multiple sessions.
Sessions last 5-10 minutes following evidence-based protocols. The app tracks training consistency and strength improvements over time. While analytics are less comprehensive than medical-grade devices, the measurements provide sufficient progress insight for most users.
What this means for you: Elvie Trainer at $199 combines award-winning design with clinical effectiveness demonstrated in systematic reviews showing pelvic floor training works for stress, urge, and mixed incontinence. Silent 5-10 minute sessions with progressive training protocols adapt to individual performance. For women who value premium aesthetics and discretion alongside evidence-based rehabilitation, this device delivers polished performance.

How Does Estrogen Deficiency Change Pelvic Floor Tissue Properties?
Estrogen receptors throughout pelvic tissues mean that declining hormone levels affect multiple structural components. Understanding these changes helps explain why pelvic floor problems increase during menopause and why rehabilitation becomes more challenging.
Collagen represents a critical structural protein in connective tissue. Estrogen stimulates collagen production and maintains existing collagen integrity. When estrogen levels drop, collagen synthesis decreases while collagen degradation accelerates. This imbalance weakens fascial supports, ligaments, and other connective structures.
Research demonstrates that hormonal changes affect tissue properties throughout the body. Studies examining estrogen deficiency effects show impacts on multiple systems including connective tissue, muscle function, and vascular health.
Several tissue property changes occur with estrogen deficiency:
Muscle fiber composition shifts toward smaller, less powerful fibers. Type I slow-twitch fibers and Type II fast-twitch fibers both decrease in size. This atrophy reduces both sustained muscle tone and rapid contraction strength.
Elastic fiber degradation reduces tissue stretch capacity. Elastin fibers that allow tissues to stretch and return to original shape deteriorate. Loss of elasticity affects vaginal tissue and supportive structures, contributing to prolapse risk.
Vascular changes reduce blood flow to pelvic tissues. Estrogen promotes healthy blood vessel function and angiogenesis. Without adequate estrogen, tissue perfusion decreases, limiting nutrient and oxygen delivery to muscles.
Nerve receptor sensitivity changes as estrogen-dependent neurological pathways adapt. Women may experience altered sensation or difficulty perceiving muscle contractions. This sensory change complicates voluntary muscle training.
Inflammatory responses increase with estrogen deficiency. Research shows that estrogen has properties that support tissue health. When levels decline, tissue repair capacity may be affected.
These interconnected changes create a challenging environment for pelvic floor health. Weakened connective tissue provides less support. Smaller muscle fibers generate less force. Reduced elasticity limits functional capacity. Altered sensation complicates rehabilitation efforts.
Understanding these mechanisms helps explain why multiple symptoms often occur together. Genitourinary syndrome of menopause encompasses various symptoms including urinary incontinence, urgency, frequency, and discomfort. The shared underlying cause - estrogen deficiency affecting multiple tissue types - produces this symptom cluster (PubMed 37019140).
Pelvic floor training works by strengthening muscles through repeated contractions. This mechanical stimulus promotes muscle protein synthesis and neural adaptation. While training cannot reverse all hormonal effects, it can counteract muscle atrophy and improve functional capacity.
The tissue changes also explain why consistency matters. Without ongoing training stimulus, menopausal pelvic floor muscles tend toward atrophy. Regular exercise maintains muscle mass and strength despite continuing estrogen deficiency. For women interested in comprehensive approaches to managing menopausal changes, our guide to menopause hot flash supplements explores additional evidence-based interventions.
A randomized trial examining pelvic floor muscle training in postmenopausal women found that training increased muscle strength more in women not using hormone therapy compared to those using it. This finding suggests that pelvic floor exercise provides meaningful benefits even without hormonal support (PubMed 29914808). Women unable or unwilling to use hormone replacement therapy can still achieve significant improvements through consistent muscle training.
What Role Does Pelvic Floor Training Play in Genitourinary Syndrome of Menopause?
Genitourinary syndrome of menopause describes a constellation of symptoms affecting the urinary and genital systems due to estrogen deficiency. This syndrome affects approximately half of all postmenopausal women, though many do not report symptoms to healthcare providers.
Symptoms include vaginal dryness, burning, irritation, dyspareunia, urinary urgency, frequency, recurrent infections, and stress or urge incontinence. These varied symptoms reflect the widespread distribution of estrogen receptors in pelvic tissues.
A 2023 review examined pelvic floor muscle rehabilitation as a treatment for genitourinary syndrome of menopause. Researchers noted that this approach represents a low-cost conservative management option with no side effects. Evidence supports using pelvic floor training alone or combined with other treatments to reduce symptoms (PubMed 37019140).
Pelvic floor training addresses several syndrome components:
Urinary incontinence improves with stronger pelvic floor muscles. Both stress incontinence (leakage with coughing, sneezing, or exertion) and urge incontinence (sudden strong urge to urinate) respond to muscle training. Strengthened muscles provide better urethral support and bladder control.
The 2022 systematic review demonstrated that a clear majority of women receiving pelvic floor muscle training significantly reduced urinary incontinence or achieved continence. Among those showing improvement, roughly half had measurable reductions in leakage episodes, while about one in five became fully continent (PubMed 35270480).
Urgency and frequency may decrease with improved muscle tone. Strong pelvic floor muscles help manage inappropriate bladder contractions. This improved control can reduce the frequency of urgent bathroom trips.
Pelvic organ support improves as muscles strengthen. While training cannot reverse severe prolapse, it can stabilize mild cases and reduce the risk of progression. Stronger muscles provide better support for pelvic organs.
Sexual function may benefit from improved muscle tone and awareness. Research suggests that pelvic floor muscle training may help reduce dyspareunia and improve sexual satisfaction. Enhanced muscle control and blood flow contribute to these improvements.
Quality of life increases when bothersome symptoms decrease. Women who successfully manage incontinence or prolapse symptoms report better social engagement, physical activity participation, and overall well-being.
The review emphasizing pelvic floor rehabilitation’s role in genitourinary syndrome treatment suggests that this approach should be part of comprehensive management plans. While vaginal estrogen therapy remains an important treatment option, not all women can or wish to use hormone therapy. Pelvic floor training provides an alternative approach.
Combining treatments may offer advantages for some women. Using both vaginal estrogen to improve tissue quality and pelvic floor training to strengthen muscles addresses different aspects of the syndrome. Healthcare providers can help women determine whether single-modality or combined approaches suit their situations.
The low-cost profile with no side effects makes pelvic floor training an appropriate first-line approach. Women can begin training while awaiting specialist appointments or trying other interventions. Early training may reduce symptom progression even if additional treatments become necessary later.
Research also indicates that pelvic floor rehabilitation works across different age ranges. While the 2023 review focused on postmenopausal women, similar approaches help younger women with pelvic floor dysfunction. This broad applicability suggests robust mechanisms underlying training effectiveness.
How Often Should Menopausal Women Use Pelvic Floor Trainers?
Training frequency significantly influences results. Most research protocols and device manufacturers recommend 3-5 sessions per week for initial strength building. This frequency balances adequate training stimulus with necessary recovery time.
The 2024 vaginal trainer study in menopausal women used regular training sessions over several weeks. While the published abstract does not specify exact frequency, the protocol produced measurable electromyographic changes in pelvic floor muscles (PubMed 38536803). This finding confirms that consistent training creates physiological adaptations.
The 2022 systematic review analyzed multiple training protocols across 15 randomized controlled trials. Studies showing the best outcomes consistently implemented regular training schedules rather than sporadic sessions. The high success rate in reducing or eliminating incontinence reflects results from consistent training programs (PubMed 35270480).
Several factors influence optimal training frequency:
Baseline muscle strength affects recovery needs. Women with severely weakened muscles may need more frequent sessions initially to create sufficient training stimulus. Those with moderate weakness might progress well with standard 3-4 times weekly schedules.
Device type influences appropriate frequency. Electrical stimulation devices like Yarlap typically recommend 3-4 sessions weekly, with each session lasting 20 minutes. Biofeedback devices often suggest 4-5 shorter sessions weekly, capitalizing on the active nature of voluntary exercises.
Individual recovery capacity varies among women. Some recover quickly between sessions and can train more frequently. Others need longer recovery periods, especially when starting training. Women should monitor for excessive soreness or fatigue indicating inadequate recovery.
Training phase determines frequency needs. Initial strength-building phases may require 4-5 sessions weekly. Maintenance phases after achieving strength goals might reduce to 2-3 weekly sessions.
Most women notice initial improvements within 4-8 weeks of consistent training.
A 2015 clinical trial tested pelvic floor muscle training programs across different groups including 38 postmenopausal women. The intervention consisted of three weekly sessions for 10 total sessions. Results showed significant increases in pelvic floor muscle strength measured by digital palpation, electromyography, and vaginal dynamometry, with concurrent decreases in urinary symptoms (PubMed 25994627). This evidence confirms that relatively short training programs can produce measurable improvements. These early changes typically include better bladder control, reduced urgency, or improved awareness of pelvic floor muscles. Continued training beyond this initial period produces further strength gains.
Long-term maintenance requires ongoing training. Unlike strength gains in hormone-stable populations, menopausal women face continuing estrogen deficiency effects. Without regular training, muscles tend toward atrophy. Maintaining 2-3 sessions weekly helps preserve gains indefinitely.
Session timing matters less than consistency. Some women prefer daily short sessions, while others prefer longer sessions spread throughout the week. Either pattern can work as long as total weekly training volume remains adequate.
Rest days between training sessions allow muscle adaptation. Pelvic floor muscles, like all skeletal muscles, strengthen during recovery periods between training sessions. Adequate rest supports positive adaptations while reducing the risk of overtraining.
Women should increase training frequency or intensity gradually. Starting too aggressively can cause muscle soreness, discouragement, or temporary symptom worsening. Beginning with 2-3 weekly sessions and gradually increasing as comfort improves promotes sustainable progress.
Tracking training frequency helps maintain consistency. Many apps record session dates automatically. For devices without tracking features, keeping a simple calendar log ensures women meet their training goals. Consistency produces better results than sporadic intense training periods. For additional support with bone health during menopause, consider evidence-based calcium and vitamin D supplementation alongside pelvic floor training.
Can Pelvic Floor Trainers Help With Both Stress and Urge Incontinence?
Menopausal women often experience mixed incontinence, with both stress and urge components. Understanding how pelvic floor training addresses different incontinence types helps women choose appropriate devices and set realistic expectations.
Stress incontinence involves urine leakage during activities that increase abdominal pressure. Coughing, sneezing, laughing, lifting, or exercising can trigger leakage. This type results from inadequate urethral support and closure. Weakened pelvic floor muscles cannot maintain sufficient urethral compression during pressure increases.
Pelvic floor training directly addresses stress incontinence mechanisms. Stronger muscles provide better urethral support. Improved muscle tone increases resting urethral pressure. Enhanced muscle coordination allows rapid contractions before pressure-increasing events. These adaptations reduce or eliminate stress incontinence episodes.
Research confirms pelvic floor training effectiveness for stress incontinence. Multiple studies demonstrate reduced leakage frequency and improved quality of life measures. The FDA clearance for Yarlap specifically includes stress incontinence treatment, indicating regulatory acceptance of evidence supporting this use.
The 2022 systematic review found that pelvic floor muscle training effectively reduced stress urinary incontinence across multiple study populations. More than six in ten women experienced significant improvements in stress incontinence specifically (PubMed 35270480).
Urge incontinence involves sudden, strong urges to urinate followed by involuntary leakage. This type results from inappropriate bladder muscle contractions. Overactive bladder muscles contract before the bladder is full, creating urgent sensations and potential leakage.
Pelvic floor training helps urge incontinence through different mechanisms than stress incontinence. Strong pelvic floor contractions can manage inappropriate bladder contractions. This “urge suppression” technique involves contracting pelvic floor muscles when urgency occurs. The muscle contraction sends neurological signals that may affect bladder muscle activity.
Evidence for urge incontinence treatment appears in the 2020 review of postmenopausal urge incontinence. The review noted that bladder training and core-stabilizing exercises represent appropriate approaches (PubMed 32267759). Pelvic floor muscles form part of the core stabilization system.
Mixed incontinence combines both stress and urge components. Research indicates that roughly half of women over 50 have pelvic organ prolapse, often accompanied by urinary incontinence (PubMed 36602196). Many of these women experience mixed incontinence rather than pure stress or urge types.
Pelvic floor training addresses mixed incontinence by targeting both contributing mechanisms. Strengthened muscles improve stress incontinence through better urethral support. The same muscles help manage urge incontinence through mechanisms affecting bladder activity. This dual action explains why training works for mixed incontinence.
Device selection may depend on primary incontinence type. Women with predominantly stress incontinence might prefer electrical stimulation devices that strengthen muscles automatically. Those with significant urge components might benefit from biofeedback devices that teach muscle control techniques.
Some women respond better to training for one incontinence type than another. Stress incontinence typically shows more predictable improvement with muscle strengthening. Urge incontinence may require additional behavioral modifications like bladder training schedules alongside pelvic floor exercises.
Treatment timelines differ between incontinence types. Stress incontinence improvements often appear within 4-6 weeks of consistent training. Urge incontinence may take 8-12 weeks to show significant changes as adaptations require more time than muscle strengthening alone.
Women with severe incontinence affecting quality of life should consult healthcare providers before relying solely on pelvic floor trainers. While training helps many women, some cases require additional interventions. Combined approaches using training, behavioral modifications, and possibly medical treatments produce best results for severe cases.
What Should Menopausal Women Look for When Choosing a Pelvic Floor Trainer?
Several factors influence which device best suits individual needs. Evaluating these considerations helps women select trainers matching their preferences, capabilities, and goals.
Technology type represents the primary decision point. Electrical stimulation devices automatically contract muscles, while biofeedback devices require voluntary engagement with real-time performance feedback. Women who struggle with muscle awareness or engagement may prefer electrical stimulation. Those who can identify and contract pelvic floor muscles might prefer biofeedback’s active involvement.
FDA clearance or CE marking indicates regulatory review. FDA-cleared devices have met safety and effectiveness standards for medical use. CE-marked devices comply with European medical device regulations. These certifications distinguish medical devices from general wellness products lacking clinical evidence.
Comfort and fit affect consistent use. Probe designs vary in size, shape, and flexibility. Silicone construction generally provides comfortable insertion. Women should verify that probe dimensions suit their anatomy, especially if vaginal tissue changes have occurred during menopause.
App requirements matter for smartphone-dependent devices. Most biofeedback trainers require compatible iOS or Android devices for functionality. Women without smartphones or those preferring device independence should choose standalone options like Yarlap.
Session duration influences daily logistics. Electrical stimulation sessions typically last 15-20 minutes. Biofeedback sessions run 5-10 minutes. Women with limited time might prefer shorter sessions, while those seeking passive training might not mind longer durations.
Progress tracking varies among devices. Some offer detailed analytics showing strength improvements, training consistency, and goal achievement. Others provide basic feedback through LED indicators or simple app displays. Women motivated by data should choose devices with comprehensive tracking.
Gamification appeal differs among users. Some women enjoy game-based training that makes exercises entertaining. Others prefer straightforward protocols without game elements. Personal preference should guide this choice, as enjoyment affects long-term consistency.
Price considerations span from $149 to $299 for quality devices. Budget constraints may limit options, but investing in effective devices provides better value than purchasing ineffective cheaper alternatives. Many insurance plans cover pelvic floor devices with healthcare provider prescriptions.
Noise levels matter for discretion. Most modern devices operate silently, but some provide auditory feedback. Women living with others or preferring quiet training should verify noise characteristics.
Battery type affects long-term costs. Rechargeable batteries eliminate ongoing replacement expenses. USB charging provides convenience for most users.
Medical conditions may influence appropriate choices. Women with certain neurological conditions, pacemakers, or other medical devices should consult healthcare providers before using electrical stimulation. Biofeedback devices generally have fewer contraindications.
Learning curve varies among devices. Simple electrical stimulation devices require minimal learning - insert, select intensity, and start. Complex biofeedback systems may require time to understand app interfaces and training programs. Tech-comfortable women may not mind learning curves, while others prefer intuitive designs.
Company reputation and support influence user experience. Established companies typically provide better customer service, warranty support, and replacement parts availability. Reading user reviews reveals actual customer experience beyond marketing claims.
Women should also consider training goals. Those primarily seeking incontinence improvement might prioritize clinical effectiveness over features. Women interested in comprehensive pelvic health might prefer devices offering varied training programs and detailed progress data. Learn more about selecting appropriate devices in our comprehensive Elvie Trainer review, which explores features relevant to menopausal users.
How Do Age-Related Changes Beyond Menopause Affect Pelvic Floor Function?
While estrogen deficiency drives major menopausal pelvic floor changes, other age-related factors also contribute. Understanding these additional influences provides complete context for rehabilitation challenges.
General muscle mass declines with aging through a process called sarcopenia. Research shows that muscle fiber number and size both decrease after age 50. This age-related atrophy affects all skeletal muscles, including pelvic floor muscles. The combination of estrogen deficiency and general aging creates compounding effects.
Collagen quality changes throughout the body with age. Cross-linking increases while flexibility decreases. These changes affect connective tissue properties in pelvic floor fasciae and ligaments. Even with adequate estrogen, aging itself alters collagen characteristics.
Nerve function changes affect muscle control and sensation. Peripheral nerve conduction slows with age. Sensory perception often decreases. These neurological changes can impair pelvic floor muscle awareness and coordination, making voluntary exercises more challenging.
Circulation changes reduce tissue perfusion throughout the body. Smaller capillary networks and reduced blood vessel elasticity limit nutrient delivery to muscles. Pelvic floor muscles receive less oxygen and nutrients for repair and maintenance.
Comorbid conditions become more common with age. Diabetes, obesity, respiratory conditions, and other health issues affect pelvic floor function. Chronic coughing stresses pelvic floor muscles. Obesity increases intra-abdominal pressure. These factors compound menopausal changes.
Previous pregnancies and deliveries create cumulative effects. Vaginal deliveries can stretch or damage pelvic floor muscles and nerves. Multiple pregnancies increase risk. These historical factors combine with menopausal changes to worsen symptoms.
Medication effects become more complex as women age. Diuretics, alpha-blockers, and other medications can affect bladder function and incontinence. Polypharmacy increases the likelihood of medication-related urinary symptoms.
Activity levels often decrease with age. Reduced physical activity leads to general deconditioning. Weaker core muscles provide less support for pelvic floor function. Sedentary lifestyles compound muscle weakness.
Despite these multiple age-related challenges, research confirms that pelvic floor training remains effective. The 2024 vaginal trainer study included menopausal women and demonstrated measurable muscle improvements (PubMed 38536803). Older muscles can still strengthen with appropriate training.
The 2022 systematic review included women across various age ranges and demonstrated consistent effectiveness. The majority of women reduced urinary incontinence across age groups, confirming that pelvic floor training works despite aging-related challenges (PubMed 35270480).
The key implication is that menopausal women should not assume age makes rehabilitation futile. While multiple factors create challenges, targeted training can counteract many negative effects. Consistency and appropriate exercise selection matter more than age itself.
Women may need to adjust expectations based on baseline function and age-related changes. Dramatic improvements seen in younger populations may not occur. However, meaningful functional gains remain achievable. Reduced incontinence frequency, improved urgency control, and better quality of life represent realistic goals.
Combining pelvic floor training with overall fitness maintenance provides additional benefits. Core strengthening, flexibility work, and cardiovascular exercise all support pelvic health. Comprehensive approaches address multiple age-related factors simultaneously. For women managing joint pain during perimenopause and menopause, evidence-based supplementation may complement pelvic floor training.
What Lifestyle Factors Support Pelvic Floor Training Effectiveness During Menopause?
Pelvic floor training works best within a supportive lifestyle context. Several modifiable factors enhance training results and overall pelvic health.
Body weight significantly affects pelvic floor stress. Excess weight increases intra-abdominal pressure, placing constant strain on pelvic floor muscles. Research shows that obesity worsens incontinence and prolapse symptoms. Even modest weight loss can reduce pelvic floor stress and improve training outcomes.
Physical activity level influences overall muscle health. Regular exercise maintains muscle mass, supports cardiovascular function, and improves tissue perfusion. However, high-impact activities may temporarily worsen symptoms during early training phases. Low-impact exercises like walking, swimming, or cycling support general fitness without excessive pelvic floor stress.
Bowel habits affect pelvic floor strain. Chronic constipation creates repetitive straining that weakens pelvic floor support. Adequate fiber intake, hydration, and regular bowel routines reduce constipation-related damage. Women should avoid prolonged straining during bowel movements.
Fluid management requires balance. Adequate hydration supports overall health, but excessive fluid intake increases bathroom frequency. Limiting caffeine and alcohol reduces bladder irritation. Evening fluid restriction may decrease nighttime urination frequency.
Smoking cessation benefits pelvic floor health through multiple mechanisms. Chronic coughing from smoking repeatedly stresses pelvic floor muscles. Smoking also impairs collagen synthesis and tissue healing. Quitting smoking removes this source of tissue damage and repetitive strain.
Lifting technique addresses acute pelvic floor stress. Proper lifting mechanics involve engaging core muscles, including pelvic floor, before lifting. Exhaling during exertion rather than holding breath reduces intra-abdominal pressure spikes.
Clothing choices can affect comfort during training. Tight clothing may interfere with device placement or create discomfort during sessions. Comfortable, loose clothing facilitates relaxed training sessions.
Sleep quality supports muscle recovery and adaptation. Poor sleep impairs tissue repair and protein synthesis. Women experiencing menopausal sleep disturbances should address sleep issues as part of comprehensive health management.
Stress management influences muscle tension patterns. Chronic stress often creates pelvic floor muscle tension and coordination problems. Relaxation techniques, mindfulness, or counseling may improve pelvic floor function for women with stress-related tension.
Nutrition quality supports muscle health and tissue repair. Adequate protein intake provides building blocks for muscle protein synthesis. Foods rich in various nutrients may support tissue quality. Calcium and vitamin D support bone health, indirectly affecting pelvic floor support structures.
Hydration timing can reduce urgency episodes. Spacing fluid intake throughout the day rather than consuming large amounts at once may decrease sudden bladder filling and urgency.
Medication review with healthcare providers identifies drugs potentially affecting bladder function. Some medications increase urination frequency or affect muscle function. Adjusting medications when medically appropriate may improve symptoms.
Sexual activity can complement pelvic floor training. Regular sexual activity involves pelvic floor muscle engagement and may help maintain muscle tone and blood flow. Women experiencing dyspareunia should address this symptom as it may indicate tissue changes requiring treatment.
Patience and consistency represent crucial behavioral factors. Pelvic floor changes took years to develop and require weeks or months to improve. Women who maintain consistent training despite slow initial progress achieve better long-term results than those who abandon training prematurely.
Creating supportive daily habits amplifies training device effectiveness. Women addressing multiple factors simultaneously often see faster, more comprehensive improvements than those focusing solely on isolated exercises.
What Are Common Mistakes to Avoid When Using Pelvic Floor Trainers During Menopause?
Understanding common training errors helps women maximize device effectiveness and avoid frustration or injury.
Starting at excessive intensity levels represents a frequent mistake. Women eager for quick results may begin electrical stimulation at uncomfortably high settings or attempt advanced biofeedback programs before building basic strength. This approach can cause muscle soreness, discouragement, or temporary symptom worsening. Starting at lower levels and progressing gradually produces better long-term results.
Inconsistent training schedules undermine results. Sporadic training provides insufficient stimulus for muscle adaptation. Women who train intensively for a week then skip several weeks see minimal improvement. Maintaining 3-5 weekly sessions, even during busy periods, ensures consistent progress.
Incorrect muscle engagement reduces biofeedback device effectiveness. Many women unconsciously contract abdominal, gluteal, or thigh muscles instead of pelvic floor muscles. This error wastes effort on ineffective contractions. Biofeedback helps identify correct muscles, but women should pay careful attention to which muscles they engage.
Rushing through contractions limits training effectiveness. Quick, jerky contractions provide less benefit than slow, sustained contractions. Most protocols recommend holding contractions for 3-10 seconds followed by equal rest periods. Maintaining proper timing throughout sessions maximizes strength gains.
Abandoning training after initial improvements allows symptom recurrence. Some women stop training once symptoms improve, assuming gains are permanent. Without ongoing maintenance training, muscles tend toward atrophy, especially given continuing estrogen deficiency. Reducing to 2-3 weekly maintenance sessions preserves long-term results.
Using inadequate lubrication creates insertion discomfort. Vaginal dryness during menopause makes device insertion more uncomfortable without proper lubrication. Using water-based lubricants compatible with silicone devices improves comfort and encourages consistent use.
Neglecting device cleaning risks infections. Improper cleaning allows bacterial growth on device surfaces. Following manufacturer cleaning instructions after each use maintains hygiene and device longevity.
Expecting immediate results leads to premature discouragement. Most women notice initial improvements within 4-8 weeks, but maximal gains may require several months. Unrealistic expectations about rapid results cause some women to abandon effective training prematurely.
Training through pain indicates improper technique or excessive intensity. Mild sensation during electrical stimulation is normal, but pain signals problems. Women experiencing pain should reduce intensity, check device positioning, or consult healthcare providers.
Ignoring other symptoms delays necessary medical care. While pelvic floor training helps many women, some symptoms indicate conditions requiring medical evaluation. Sudden symptom changes, pain, bleeding, or severe prolapse warrant professional assessment.
Focusing solely on device training while ignoring supportive lifestyle factors limits results. Continuing behaviors that stress pelvic floors - chronic coughing, constipation, excessive weight, high-impact exercise - undermines training efforts. Comprehensive approaches addressing multiple factors produce better outcomes.
Comparing progress to others creates unrealistic expectations. Individual results vary based on baseline strength, hormonal status, age, and other factors. Some women see dramatic improvements quickly, while others progress more gradually. Focusing on personal progress rather than comparisons maintains motivation.
Skipping healthcare provider consultations when needed delays diagnosis of conditions affecting training effectiveness. Women with moderate to severe prolapse, neurological conditions, or other complications may need professional guidance for safe, effective training.
Avoiding these common errors helps women achieve optimal results from pelvic floor training devices while maintaining safety and comfort throughout rehabilitation.
How Can Women Track Progress With Pelvic Floor Training During Menopause?
Objective progress tracking provides motivation and helps women recognize improvements that might otherwise go unnoticed. Several methods allow comprehensive progress assessment.
Symptom journaling creates baseline records and tracks changes. Women should record incontinence episode frequency, urgency severity, pad usage, and quality of life impacts before starting training. Weekly updates reveal gradual improvements that might not be obvious day-to-day.
Tracking metrics include:
- Number of leakage episodes per day or week
- Urgency severity on 1-10 scale
- Number of pads used daily
- Activities that trigger leakage
- Nighttime bathroom frequency
- Subjective symptom severity ratings
Device-recorded data provides objective strength measurements. Biofeedback apps automatically track contraction strength, session frequency, and program progression. Reviewing weekly or monthly trends shows strength gains over time.
Pad weight testing offers measurable leakage quantification. Women can weigh pads before and after wearing to calculate exact leakage volume. This precise measurement reveals gradual reductions that might not be subjectively obvious.
Quality of life assessments measure functional improvements. Validated questionnaires like the International Consultation on Incontinence Questionnaire (ICIQ) provide standardized symptom severity measures. Repeating assessments every 4-8 weeks shows improvement trends.
Activity participation tracking reveals functional gains. Many women with incontinence limit social activities, exercise, or travel due to symptom concerns. Gradually resuming previously avoided activities indicates real-world improvement.
Photography or mirror checks document prolapse changes for women with visible prolapse. While not appropriate for everyone, some women find visual documentation helpful for tracking mild prolapse reduction.
Healthcare provider assessments offer professional evaluation. Pelvic floor physical therapists can perform internal examinations measuring muscle strength using standardized grading scales. Professional assessments every 8-12 weeks provide expert progress evaluation.
The 2022 systematic review noted that most studies used pad tests, bladder diaries, and quality of life questionnaires to measure outcomes (PubMed 35270480). These same tools work for individual progress tracking at home.
Realistic timelines help interpret progress appropriately. Research shows most women notice initial improvements within 4-8 weeks, with continued gains over 3-6 months. Understanding typical timelines reduces premature discouragement from gradual progress.
Celebration of small wins maintains motivation during gradual improvement phases. Reducing from 5 daily leakage episodes to 3 represents meaningful progress even though symptoms persist. Recognizing incremental improvements encourages continued training.
Regular progress review helps women stay motivated through rehabilitation challenges while providing objective evidence of training effectiveness.
Complete Support System for Menopausal Pelvic Floor Health
Comprehensive pelvic floor care extends beyond device use. A multi-faceted approach addresses various aspects of menopausal genitourinary health.
Professional assessment establishes baseline function and identifies specific problems. Pelvic floor physical therapists can evaluate muscle strength, coordination, and dysfunction patterns. This professional input guides training approaches and identifies cases requiring additional interventions.
Vaginal moisturizers address tissue dryness that may interfere with device comfort. Regular moisturizer use maintains tissue hydration between training sessions. This lubrication support complements muscle training.
Water-based lubricants facilitate comfortable device insertion. Women should verify that lubricants are compatible with silicone devices. Adequate lubrication reduces tissue irritation during training.
Device cleaning protocols maintain hygiene and device longevity. Most manufacturers recommend washing with mild soap and water after each use. Some devices come with specialized cleaning solutions. Proper cleaning reduces infection risk.
Storage solutions protect devices between uses. Many trainers include storage cases that maintain hygiene and discretion. Clean, dry storage reduces contamination risk.
Bathroom habits deserve attention alongside training. Avoiding “just in case” urination helps maintain normal bladder capacity. Responding to urgency with pelvic floor contractions rather than immediate bathroom trips builds control.
Incontinence products provide security during training phases. Reusable or disposable pads reduce embarrassment during symptom improvement. Women should not view pad use as training failure but rather as temporary support during rehabilitation.
Support groups offer emotional support and practical advice. Many women feel isolated dealing with pelvic floor problems. Connecting with others facing similar challenges reduces stigma and provides encouragement.
Educational resources help women understand pelvic floor anatomy and function. Better knowledge improves exercise technique and treatment compliance. Reputable sources include professional organizations and evidence-based health websites.
Healthcare provider coordination ensures comprehensive care. Women should inform gynecologists, primary care physicians, and specialists about pelvic floor training. Providers can adjust other treatments to complement training efforts.
Symptom tracking reveals patterns and progress. Keeping logs of incontinence episodes, urgency frequency, and pad use provides objective improvement measures. These records help women recognize gradual progress that might otherwise go unnoticed.
Realistic expectations support long-term commitment. Most women see initial improvements within 4-8 weeks, but maximal gains may require several months. Understanding typical timelines helps maintain motivation through early phases.
Long-term commitment to maintenance training supports lasting results. After achieving initial goals, ongoing 2-3 weekly sessions preserve gains. Viewing pelvic floor training as permanent rather than temporary produces lasting results.
Backup plans for device issues maintain training continuity. Women should know how to contact manufacturers for technical support or warranty service. Having troubleshooting resources available maintains training consistency.
Travel accommodations allow training continuation away from home. Portable devices, USB charging, and hygiene supplies enable training during travel. Maintaining routines during trips reduces the risk of regression.
This comprehensive support framework maximizes training effectiveness while addressing practical, emotional, and logistical aspects of pelvic floor rehabilitation. Women who build complete support systems achieve better outcomes than those using devices in isolation.
Frequently Asked Questions
Why does menopause affect pelvic floor muscles?
Estrogen decline during menopause reduces collagen production and muscle tone in pelvic floor tissues. Research shows that estrogen deficiency has both direct and indirect effects on muscle quality, affecting the body’s ability to repair and maintain muscle tissue. This hormonal shift contributes to weakened pelvic support structures and increased risk of incontinence.
How long does it take for pelvic floor trainers to show results during menopause?
Most studies report noticeable improvements within 4-8 weeks of consistent use. A 2024 study using vaginal trainers in menopausal women showed measurable changes in electromyographic activity of pelvic floor muscles after regular use. Results depend on baseline muscle strength, frequency of use, and individual hormonal factors.
Can pelvic floor trainers replace hormone replacement therapy for incontinence?
Pelvic floor muscle training is a complementary approach rather than a replacement for hormone therapy. Research indicates that pelvic floor rehabilitation works well alone or in combination with other treatments for genitourinary syndrome of menopause. Women should discuss comprehensive treatment options with their healthcare provider to address both hormonal and muscular factors.
Are electronic stimulation devices better than manual Kegel exercises for menopausal women?
Electronic stimulation devices may offer advantages for women who struggle with proper muscle engagement. Research shows that electrical muscle stimulation can activate pelvic floor muscles automatically, which helps women who cannot identify or contract the correct muscles voluntarily. Both approaches have evidence supporting their effectiveness.
Do pelvic floor trainers help with vaginal dryness during menopause?
Pelvic floor trainers primarily strengthen muscles rather than directly treating vaginal dryness. However, a 2023 review noted that pelvic floor muscle rehabilitation may help improve some symptoms of genitourinary syndrome of menopause when used with other treatments. Increased blood flow from muscle contractions may provide secondary benefits for tissue health.
What is the best frequency for using pelvic floor trainers during menopause?
Most manufacturers and research protocols recommend 3-5 sessions per week for optimal results. The 2024 vaginal trainer study in menopausal women used regular training sessions over several weeks. Consistency matters more than duration, with 10-15 minute sessions typically sufficient for most devices.
Can pelvic floor trainers help with pelvic organ prolapse in menopausal women?
Research indicates that roughly half of women over 50 have pelvic organ prolapse. Pelvic floor muscle training can help strengthen supportive structures, potentially reducing mild prolapse symptoms. However, women with moderate to severe prolapse should consult a healthcare provider before starting any exercise program, as some cases may require additional interventions.
Are app-based biofeedback trainers more effective than simpler devices?
Biofeedback devices provide real-time information about muscle contraction quality and strength, which may improve technique and motivation. Studies show that proper muscle engagement is crucial for effectiveness. While simpler devices work well for some women, biofeedback can help ensure correct form, especially for those new to pelvic floor training.
Do I need to use a pelvic floor trainer indefinitely during menopause?
Long-term maintenance is typically recommended to preserve gains. After initial strength improvements, many women reduce frequency to 2-3 sessions weekly for maintenance. Since estrogen levels remain low after menopause, ongoing muscle training helps counteract continued hormonal effects on tissue quality.
Can pelvic floor trainers improve sexual function during menopause?
Research indicates that stronger pelvic floor muscles are associated with improved sexual function. A 2023 review noted that pelvic floor rehabilitation may help reduce symptoms affecting sexual activity, including dyspareunia. Improved muscle tone and blood flow from regular training may support various aspects of sexual health.
Our Top Recommendations
After reviewing research evidence and product specifications, device selection depends on individual needs based on individual needs and preferences.
Best Overall: Yarlap with AutoKegel delivers FDA-cleared electrical muscle stimulation for women who need automatic training without requiring voluntary muscle engagement. The device’s 20 intensity levels and clinical-grade protocols make it ideal for menopausal women struggling with muscle awareness or seeking consistent results without technique variables.
Best Budget: Perifit offers proven biofeedback technology with extensive gamification at an accessible $149 price point. This device suits women who want engaging, interactive training with real-time feedback but need to manage costs. The combination of games and structured exercise programs provides training variety.
Best for Biofeedback: Perifit Care+ provides medical-grade sensors with comprehensive analytics for women who value detailed progress data. The sophisticated tracking and personalized programs justify the higher price for users wanting thorough insight into their pelvic floor rehabilitation.
Premium Pick: Elvie Trainer combines clinical effectiveness with award-winning design and silent operation. This device appeals to women who prioritize aesthetics, discretion, and refined user experience alongside evidence-based training protocols.
All four devices offer effective pelvic floor training for menopausal women. Choice depends on personal preferences regarding automation versus active engagement, data detail, gamification, and budget considerations.
Join the discussion: Facebook | X | YouTube | Pinterest
Conclusion
Menopause creates significant challenges for pelvic floor health through estrogen deficiency, muscle atrophy, and connective tissue changes. Research confirms that nearly half of postmenopausal women experience pelvic floor dysfunction, including urinary incontinence and pelvic organ prolapse.
Evidence-based pelvic floor training provides effective intervention for these menopausal changes. Studies demonstrate that both electrical stimulation and biofeedback approaches produce measurable improvements in muscle function and symptom reduction. The technology works by strengthening weakened muscles, improving neuromuscular coordination, and enhancing voluntary control.
Device selection should match individual needs, capabilities, and preferences. Electrical stimulation devices like Yarlap automatically contract muscles, bypassing voluntary engagement challenges. Biofeedback devices like Perifit, Perifit Care+, and Elvie Trainer provide real-time feedback for active training with varying levels of gamification and analytics.
Consistency matters more than device choice for long-term success. Women who maintain 3-5 weekly sessions during initial training phases, then reduce to 2-3 sessions for maintenance, achieve the best results. Combining device training with supportive lifestyle factors amplifies effectiveness.
While pelvic floor trainers cannot reverse hormonal changes, they can counteract many negative effects on muscle function. Most women notice improvements within 4-8 weeks of consistent use. Long-term commitment preserves gains despite continuing estrogen deficiency.
Women experiencing bothersome pelvic floor symptoms should recognize that age or menopause does not make improvement impossible. Research-backed training devices offer realistic hope for better bladder control, reduced urgency, and improved quality of life during the menopausal transition and beyond.
Related Reading
- Best Pelvic Floor Trainer - Comprehensive comparison of top pelvic floor training devices
- Elvie Trainer Review - In-depth analysis of Elvie’s premium biofeedback device
- Kegel Exerciser for Postpartum Recovery - Pelvic floor training principles applicable to menopausal rehabilitation
- Best Collagen Supplements for Women - Supporting connective tissue health during menopause
- Best Anti-Aging Supplements for Women in Their 30s Prevention Guide - Proactive approaches to aging-related changes
- Magnesium L-Threonate for Cognitive Function - Essential mineral for muscle function and relaxation
- Menopause Hot Flashes Supplements - Evidence-based supplements for menopausal symptoms
- Bone Health Osteoporosis Supplements Women 40 - Calcium, vitamin D, and bone support during menopause
- Joint Pain Arthritis Supplements Women 40 - Support for managing menopausal joint issues
References
Vaginal trainer increased electromyographic activity of pelvic floor muscles in menopausal women. PubMed PMID 38536803
Pelvic floor muscle rehabilitation for genitourinary syndrome of menopause - low-cost conservative management with no side effects. PubMed PMID 37019140
Kegel exercises and core stability in women over 50 - 50% of women over 50 have pelvic organ prolapse. PubMed PMID 36602196
Pelvic floor muscle training for urinary incontinence with or without biofeedback or electrostimulation - 62% of women significantly reduced urinary incontinence or achieved continence. PubMed PMID 35270480
Urge incontinence in postmenopausal women - bladder training and core-stabilizing exercises as first-line approaches. PubMed PMID 32267759
Biofeedback adds value to pelvic floor muscle training - superior improvements in muscle strength and endurance. PubMed PMID 28508398
Randomized controlled trial of pelvic floor muscle training in 40 postmenopausal women over 12 weeks. PubMed PMID 38206341
Virtual reality-based gamified pelvic floor training in 27 postmenopausal women showed significant muscle strength increases. PubMed PMID 25925487
Pelvic floor muscle training in postmenopausal women - strength increases with 10-session protocol. PubMed PMID 25994627
Pelvic floor training works even without hormone therapy in postmenopausal women. PubMed PMID 29914808
Recommended Products
Get Weekly Research Updates
New studies, updated reviews, and evidence-based health insights delivered to your inbox. Unsubscribe anytime.