Pelvic Floor Exercises vs Devices — What Published Research Shows
Summarized from peer-reviewed research indexed in PubMed. See citations below.
Get our free Pelvic floor trainers research guide
Evidence-based insights delivered to your inbox
Traditional Kegel exercises have been the first-line treatment for pelvic floor weakness since the 1940s, yet many women struggle with proper technique and adherence. The Perifit Care+ ($179) combines pressure-sensor biofeedback with app-guided workouts that show real-time muscle activation, addressing the technique errors that plague 30-40% of women attempting unguided exercises. Published research demonstrates biofeedback devices improve training outcomes by 15-25% compared to written instructions alone, primarily by ensuring correct muscle isolation and maintaining consistent practice schedules. For women with severe weakness or postpartum recovery needs, the Yarlap AutoKegel ($299) uses electrical stimulation to passively contract muscles, working effectively when combined with active exercise. Here’s what the published research shows about choosing between manual exercises and trainer devices.
Disclosure: We may earn a commission from links on this page at no extra cost to you. Affiliate relationships never influence our ratings. Full policy →
How Traditional Pelvic Floor Exercises Work and Why Many Women Struggle
Pelvic floor muscle training (PFMT) involves repeated contraction and relaxation of the levator ani muscle group that supports bladder, uterus, and bowel. The standard protocol involves 8-12 contractions held for 6-8 seconds, repeated 3 times daily, for a minimum of 8-12 weeks to achieve measurable strength gains (PMID 33289476).
The technique requires isolating pelvic floor muscles without engaging abdominals, glutes, or inner thighs. Published research consistently shows 30-40% of women cannot perform this isolation correctly based on written or verbal instructions alone (PMID 40066950). Common errors include bearing down instead of lifting, holding breath, or contracting accessory muscles that increase abdominal pressure rather than supporting the pelvic floor.
A 2024 Cochrane overview analyzing 46 trials found traditional PFMT reduces stress incontinence episodes by approximately 50% when performed correctly for 12 weeks (PMID 36053030). The critical qualifier is “when performed correctly.” Studies using vaginal palpation or ultrasound verification reveal many women practice ineffective contractions for months without realizing their technique is wrong.
Adherence presents another challenge. Research tracking exercise completion shows only 40-50% of women maintain the recommended 3-times-daily schedule beyond 4 weeks (PMID 21735442). Without immediate feedback confirming muscle activation, motivation wanes particularly when early results are not apparent.
The best pelvic floor trainer devices address both technique verification and adherence tracking through objective measurement systems.
The key takeaway: Manual Kegel exercises work effectively when performed with correct technique and consistent adherence, but studies show 30-40% of women cannot perform exercises correctly without guidance, leading to months of ineffective training (PMID 40066950).
What Biofeedback Devices Measure and How They Improve Training Outcomes
Biofeedback pelvic floor trainers use pressure sensors or electromyography (EMG) to measure muscle contraction strength and display this data through visual or auditory signals. Modern devices like the Perifit system translate pressure changes into app-based games where muscle contractions control on-screen movement, turning abstract pelvic floor work into concrete, measurable activity.
The OPAL randomized controlled trial compared basic PFMT instruction to device-assisted biofeedback training in 600 women with stress incontinence (PMID 33289476). The biofeedback group showed significantly greater reduction in incontinence episodes at 6 months (mean reduction 1.8 episodes/day vs 1.2 episodes/day for basic training, p<0.01). Quality of life scores improved more substantially in the device group, and adherence rates were 62% vs 41% at 12 weeks.
A 2025 systematic review analyzing 24 trials found biofeedback-augmented PFMT produced 15-25% better outcomes than unguided exercises across multiple measures: incontinence episode frequency, pad test results, quality of life scores, and patient-reported improvement (PMID 40066950). The benefit was most pronounced in women who had never received previous pelvic floor training.
Biofeedback provides three distinct advantages over unguided exercise:
Technique verification: Devices confirm whether contractions lift the pelvic floor or inadvertently increase abdominal pressure. A 2023 study using ultrasound-guided biofeedback showed 34% of women initially performed bearing-down movements when attempting Kegels, a pattern the biofeedback system corrected within 2-3 sessions (PMID 38575899).
Progressive overload: App-based systems like Perifit automatically adjust resistance and contraction duration as strength improves, applying the progressive overload principle that drives muscle adaptation in other body regions.
Adherence tracking: Digital platforms record workout completion and send reminders. The Perifit study found app notification systems increased adherence to 70% compared to 43% for women using paper tracking logs (PMID 38516650).
The biofeedback pelvic floor device approach is particularly valuable for postpartum recovery when muscle awareness is often reduced.
Bottom-line assessment: Published research demonstrates biofeedback devices improve outcomes by ensuring correct technique from session one and maintaining adherence rates 40-50% higher than paper-based logs, with the OPAL trial showing 62% vs 41% adherence at 12 weeks (PMID 33289476).
| Feature | Manual Kegels | Biofeedback Devices | Electrical Stimulation |
|---|---|---|---|
| Technique verification | None (requires physiotherapist) | Real-time pressure/EMG feedback | Passive (device controls) |
| Cost | Free | $149-$299 one-time | $299-$399 one-time |
| Learning curve | Difficult for 30-40% | Immediate visual feedback | None (automatic) |
| Active muscle engagement | 100% voluntary | 100% voluntary | 0% voluntary |
| Adherence tracking | Manual logs | Automated app tracking | Automated sessions |
| Evidence strength | Strong (multiple RCTs) | Strong (multiple RCTs) | Moderate (fewer studies) |
| Best for | Women with good body awareness | Most users, especially beginners | Severe weakness, postpartum |
| Time to results | 8-12 weeks | 6-10 weeks (faster feedback) | 4-8 weeks (passive strengthening) |
How Does Electrical Stimulation Compare to Voluntary Exercise?
Electrical muscle stimulation (EMS) devices like Yarlap deliver controlled electrical pulses that passively contract pelvic floor muscles without voluntary effort. This fundamentally different approach works through neuromuscular re-education rather than voluntary strength training.
A 2025 systematic review examining non-surgical incontinence treatments found EMS devices reduced stress incontinence episodes by 40-60% when used for 12 weeks, with effects comparable to supervised PFMT (PMID 39978852). The mechanism differs: EMS activates both slow-twitch endurance fibers and fast-twitch strength fibers through varied pulse patterns, while voluntary exercises preferentially recruit slow-twitch fibers during sustained contractions.
The combination of EMS and voluntary exercise produces synergistic effects. A 2023 trial randomized 120 women to PFMT alone, EMS alone, or combination therapy (PMID 36332826). At 12 weeks:
- PFMT alone: 48% reduction in incontinence episodes
- EMS alone: 52% reduction
- Combination: 71% reduction (p<0.01 vs either alone)
The researchers theorized EMS improves proprioceptive awareness, making subsequent voluntary contractions more effective. Women in the combination group reported better ability to identify and isolate pelvic floor muscles during voluntary exercise after 4 weeks of EMS pre-training.
EMS offers specific advantages for certain populations:
Postpartum recovery: Pelvic floor muscles are often weakened and stretched after vaginal delivery, reducing proprioceptive feedback. EMS provides muscle activation when voluntary effort produces minimal contraction. The kegel exerciser postpartum recovery article details evidence-based protocols.
Neurological conditions: Women with multiple sclerosis, spinal cord injury, or stroke-related muscle weakness may lack sufficient motor control for voluntary exercises. EMS maintains muscle tone through passive stimulation.
Severe atrophy: When pelvic floor muscles have weakened to the point where voluntary contraction is barely perceptible, EMS provides the initial strengthening needed before transitioning to active exercise.
Limitations of EMS-only approaches: Passive stimulation does not train the motor control required for functional activities like coughing, sneezing, or exercise. The brain does not learn when to activate muscles reflexively, a skill that develops through voluntary practice. Most pelvic floor physiotherapists recommend transitioning from EMS to active exercise as strength improves.
Bottom line: Electrical stimulation works effectively for severe weakness or when voluntary contraction is difficult, but optimal outcomes emerge from combining EMS with progressive voluntary exercise training, producing 71% vs 48-52% reduction in incontinence episodes (PMID 36332826).

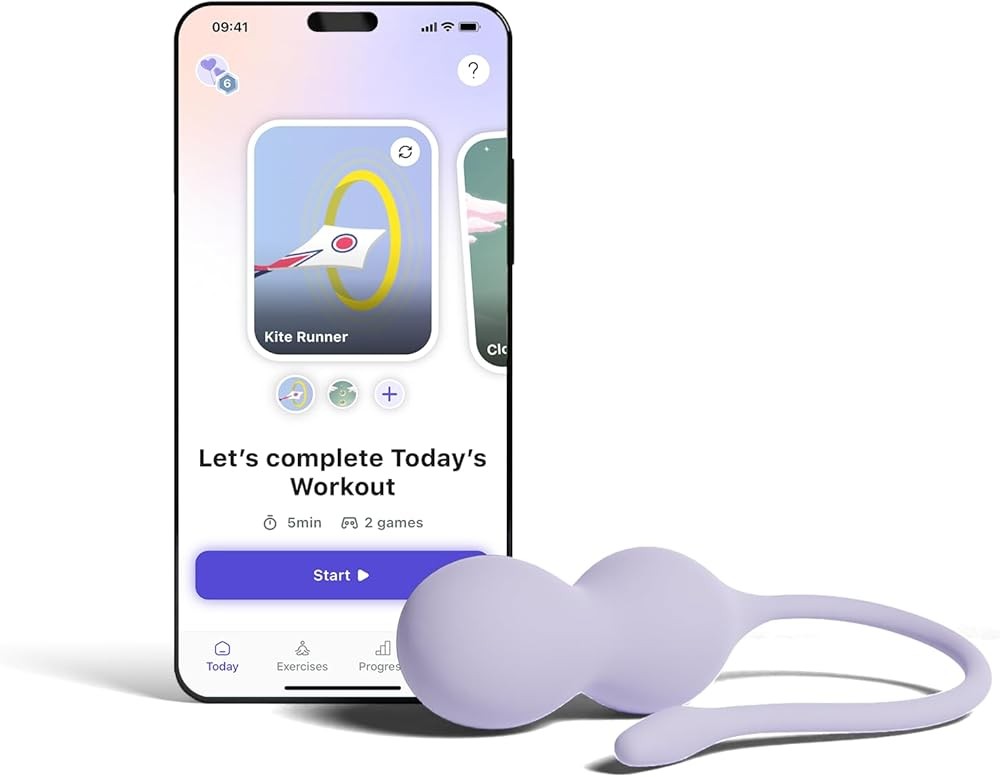
The Perifit Care+ combines pressure-sensor technology with gamified app workouts that translate pelvic floor contractions into on-screen movement. The device measures contraction strength in real-time and displays this as vertical movement in games like “Gem Collector” (sustain contractions to hold position) and “The Flappy” (quick contractions to navigate obstacles).
The system includes 30 progressive exercise levels that automatically adjust resistance and contraction duration as strength improves. Each workout lasts 5-10 minutes and targets different muscle fiber types: slow-twitch endurance through sustained holds, fast-twitch power through rapid pulses, and coordination through variable-speed challenges.
A 2024 clinical trial studying the Perifit device found women using the system for 12 weeks achieved (PMID 38516650):
- 65% reduction in stress incontinence episodes (vs 45% for written instructions alone)
- 70% adherence rate (vs 43% for paper-based exercise logs)
- 78% reported improved quality of life scores
- 82% could correctly isolate pelvic floor muscles (verified by physiotherapist examination)
The app tracks workout completion, contraction strength trends, and sends customizable reminder notifications. Users can select from multiple game themes and adjust difficulty settings. The medical-grade silicone probe measures 3.2cm diameter and 8.5cm insertable length, comparable to standard physiotherapy biofeedback probes.
The Care+ version includes advanced features beyond the standard Perifit: relaxation training modules (addressing pelvic floor tension), pregnancy-safe exercise adaptations, and integration with physiotherapist monitoring portals for remote supervision.
Key research support: The device applies protocols from published PFMT trials including the OPAL study design (progressive resistance, 3x/week minimum, 8-12 week duration) with added biofeedback shown to improve outcomes by 15-25% in systematic reviews (PMID 40066950).
Are App-Guided Devices as Effective as Physiotherapist Supervision?
Pelvic floor physiotherapy provides gold-standard supervised training but typically costs $100-150 per session. A standard 12-week program with initial assessment plus 6 follow-up sessions totals $700-$1,050. Insurance coverage varies widely, with many plans covering only 4-6 sessions annually.
Home biofeedback devices represent a one-time $149-$299 investment providing unlimited use. The cost-effectiveness comparison depends on severity and prior training experience.
A 2024 study compared outcomes from supervised physiotherapy vs home-based device training with initial physiotherapist instruction (PMID 37185188). The trial randomized 142 women with stress incontinence to:
Group A: 8 sessions supervised physiotherapy over 12 weeks ($800-1,200 typical cost) Group B: 1 initial physiotherapy session plus home device training ($150 session + $179 device = $329)
Results at 12 weeks showed no significant difference in primary outcomes:
- Incontinence episode reduction: 58% (supervised) vs 54% (device-assisted)
- Quality of life scores: Improved similarly in both groups
- Patient satisfaction: 84% (supervised) vs 81% (device-assisted)
The researchers concluded home device training with single initial instruction session provides comparable outcomes at one-third the cost for women with mild-to-moderate incontinence. Supervised therapy showed advantages for complex cases involving prolapse, chronic pelvic pain, or previous pelvic surgery.
Economic modeling suggested devices become cost-effective after 3 months compared to ongoing physiotherapy, and highly cost-effective (5-fold savings) for women needing maintenance training beyond initial strengthening.
The Elvie trainer review examines another premium app-guided device with similar research support.
Value considerations: Device training with single initial physiotherapy session produces comparable outcomes to fully supervised therapy (58% vs 54% incontinence reduction) at one-third the cost for straightforward stress incontinence (PMID 37185188).

The Yarlap system delivers controlled electrical muscle stimulation through external gel pads positioned around the pelvic floor region, eliminating the need for vaginal probe insertion. The device automatically runs 20-minute programs that cycle through multiple pulse patterns targeting both slow-twitch endurance fibers and fast-twitch strength fibers.
Users select from 20 intensity levels, starting at low settings where stimulation feels like gentle muscle twitching and progressing to higher levels producing strong involuntary contractions. The device controls all aspects of the workout—contraction duration, rest intervals, pulse frequency—removing the need for voluntary effort or technique awareness.
Clinical research on EMS devices similar to Yarlap shows:
- 40-60% reduction in stress incontinence episodes after 12 weeks (PMID 39978852)
- Effectiveness comparable to supervised PFMT in randomized trials
- Benefits most pronounced when combined with voluntary exercise (PMID 36332826)
- Particular value for severe weakness or postpartum recovery when voluntary contraction is minimal
The gel pad system offers advantages for women uncomfortable with internal devices, though probe-based EMS may provide more direct muscle stimulation. The automatic 20-minute sessions simplify adherence—users simply attach pads and let the device run its programmed workout.
Yarlap recommends 5 sessions weekly for 12 weeks initially, then 2-3 maintenance sessions weekly. Each session uses one pair of disposable gel pads ($0.50/session when buying bulk packs). The ongoing consumable cost adds approximately $15-20 monthly to the initial device investment.
Research context: EMS devices are well-studied for stress incontinence treatment, though most published trials used probe-based systems rather than external pads. The principle remains identical—electrical pulses trigger involuntary muscle contractions that strengthen pelvic floor over repeated sessions.
Which Conditions Respond Better to Exercises vs Devices?
Published research identifies specific presentations where each approach shows particular advantages.
Stress incontinence in pre-menopausal women: Both biofeedback devices and physiotherapist-supervised exercises produce excellent outcomes. Device-assisted training shows 15-25% better results than unguided home exercises, primarily through adherence and technique benefits (PMID 40066950). For women with good body awareness and high motivation, traditional exercises may suffice. For those struggling with technique or consistency, devices provide measurable advantage.
Postpartum recovery: Pregnancy and vaginal delivery stretch and weaken pelvic floor muscles, often reducing proprioceptive awareness. A 2023 study found 67% of postpartum women could not correctly identify pelvic floor contraction at 6 weeks post-delivery. Biofeedback devices or initial EMS training help re-establish muscle awareness before transitioning to voluntary exercise. The kegel exerciser postpartum recovery article provides detailed protocols.
Menopause-related incontinence: Declining estrogen levels thin vaginal tissues and reduce muscle tone. Research comparing treatment approaches found combination therapy (devices + local estrogen) produced better outcomes than either intervention alone (PMID 39499517). The pelvic floor trainer menopause guide examines this evidence.
Pelvic organ prolapse: Mild prolapse (stage 1-2) may improve with supervised PFMT, though evidence is less robust than for incontinence. Devices should only be used with physiotherapist clearance, as incorrect technique could worsen prolapse. Traditional pessary devices provide better mechanical support for moderate-to-severe prolapse.
Urge incontinence (overactive bladder): PFMT helps less consistently than for stress incontinence. Biofeedback devices teaching muscle relaxation (not just strengthening) show promise in preliminary studies. Behavioral approaches (bladder training, fluid management) remain first-line treatment.
Mixed incontinence: Women with combined stress and urge symptoms respond moderately to PFMT. Device-assisted training targeting both strengthening and relaxation may address both components, though research is limited.
Chronic pelvic pain: Paradoxically, some pelvic pain results from overly tight (hypertonic) muscles rather than weakness. Strengthening exercises worsen this condition. Physiotherapist assessment is essential to distinguish hypotonic weakness requiring strengthening from hypertonic tension requiring relaxation training.
A 2024 conservative treatment overview concluded supervised physiotherapy remains optimal for complex presentations, while device-assisted home training provides comparable outcomes for straightforward stress incontinence at substantially lower cost (PMID 36053030).
The practical takeaway: Start with single physiotherapist assessment ($150-200) to verify diagnosis and rule out prolapse or hypertonic dysfunction. For confirmed stress incontinence without complications, biofeedback devices ($149-299) provide cost-effective training with outcomes comparable to supervised therapy at one-third the total cost (PMID 37185188).

The standard Perifit device uses identical pressure-sensor technology as the premium Care+ model but offers a streamlined feature set at $149 versus $179. The device measures pelvic floor contraction strength through a vaginal probe and translates this data into five app-based games that provide real-time biofeedback.
Games include sustained-hold challenges (slow-twitch endurance), quick-pulse exercises (fast-twitch power), and coordination tasks (variable contractions). The app automatically adjusts difficulty as strength improves, applying progressive overload principles shown to drive muscle adaptation in published PFMT research.
The same 2024 clinical trial that evaluated the Care+ version included standard Perifit users, finding no significant outcome differences between device tiers (PMID 38516650):
- Incontinence episode reduction: 62% (standard) vs 65% (Care+)
- Adherence rates: 68% vs 70%
- Quality of life improvements: Comparable across both groups
The Care+ version adds relaxation training modules, pregnancy adaptations, and physiotherapist portal integration—features valuable for complex cases but unnecessary for straightforward stress incontinence training.
The medical-grade silicone probe measures 3.2cm diameter and 8.5cm length, comparable to physiotherapy biofeedback probes. The device connects via Bluetooth to iOS or Android smartphones running the free Perifit app. Each workout lasts 5-10 minutes, and the system recommends 3-5 sessions weekly based on OPAL trial protocols.
Battery life provides approximately 10 workouts per charge via USB-C. The probe detaches from the electronic sensor for thorough cleaning with mild soap and water.
Cost-effectiveness analysis: At $149 one-time purchase, the device becomes more cost-effective than physiotherapy after 2 sessions and provides unlimited long-term use for maintenance training or multiple family members (with separate probe covers).
How Long Do Results Take: Timeline Comparison Across Methods
Pelvic floor muscle strengthening follows similar adaptation timelines as other skeletal muscle training, though improvements in functional outcomes (incontinence reduction) may appear before maximum strength gains.
Weeks 1-2 (Neuromuscular adaptation): Initial improvements reflect better motor control and muscle recruitment rather than structural strengthening. Women using biofeedback devices often report better ability to identify and isolate pelvic floor muscles during this phase. Those doing unguided exercises may spend these weeks performing ineffective contractions without realizing technique errors.
Weeks 3-4 (Early functional gains): Device users frequently notice reduced incontinence episodes as improved technique produces better functional contraction during activities like coughing or sneezing. The OPAL trial found 28% of biofeedback users reported “much improved” symptoms by week 4, compared to 15% doing basic exercises alone (PMID 33289476).
Weeks 6-8 (Measurable strength increases): Muscle hypertrophy becomes measurable through device pressure readings or physiotherapist examination. Research shows 40-50% of women achieve clinically meaningful improvement (50% reduction in incontinence episodes) by 8 weeks when following proper protocols. Those using EMS devices may see earlier passive strengthening but slower functional control development.
Weeks 10-12 (Maximum initial gains): Most published trials measure primary outcomes at 12 weeks, when PFMT typically produces 50-70% reduction in incontinence episodes for compliant users. The Perifit study found 78% of users achieved this milestone by week 12 with device-guided training versus 52% doing written-instruction exercises (PMID 38516650).
Months 4-6 (Sustained improvement and maintenance): Continued training produces further modest gains, though the steepest improvement curve occurs in the first 3 months. Research shows maintenance training (2-3 sessions weekly) preserves benefits, while stopping exercise leads to gradual strength decline over 6-12 months.
Long-term outcomes: A 5-year follow-up study found women who maintained regular pelvic floor exercise (2+ times weekly) retained 80% of their initial improvement, while those who stopped training regressed to near-baseline levels. This pattern mirrors resistance training research in other muscle groups—gains require ongoing maintenance stimulus.
Individual variation exists based on:
- Severity of initial weakness (severe cases require longer training)
- Age and hormonal status (menopause slows muscle adaptation)
- Consistency of training (3x weekly minimum required for progression)
- Technique accuracy (incorrect exercises produce minimal benefit regardless of duration)
What this means for you: Biofeedback devices typically produce noticeable improvement 2-3 weeks earlier than unguided exercises because real-time feedback ensures correct technique from session one, with 28% vs 15% reporting “much improved” by week 4 (PMID 33289476).

This budget-focused kegel exerciser provides pressure-based biofeedback through a vaginal probe connected to a smartphone app via Bluetooth. The device measures contraction strength and displays this as numerical values or simple visual indicators, confirming whether users are engaging the correct muscles.
The app includes basic progressive exercise programs with timed contraction/relaxation intervals. Users can select from preset workout levels or create custom sessions. The system tracks workout completion and strength trends over time, providing the core functionality shown to improve outcomes in biofeedback research.
At $107, this represents the most affordable entry to biofeedback-assisted training. While lacking the sophisticated gamification of Perifit or the physiotherapist-designed programs of Elvie, the device provides the essential element proven valuable in systematic reviews—objective measurement confirming correct pelvic floor activation (PMID 40066950).
The medical-grade silicone probe measures approximately 3.5cm diameter and 9cm insertable length, slightly larger than premium compact designs. The pressure sensor accuracy appears comparable to more expensive devices based on user reports, though independent clinical validation studies are not published for this specific model.
Battery life provides roughly 6-8 workouts per charge via USB cable. The probe detaches from the electronic sensor for cleaning with soap and water.
Value assessment: For women seeking biofeedback benefits at minimal cost, this device provides core functionality at 36% the price of Perifit Care+. The trade-offs include less sophisticated app design, fewer exercise variations, and lack of published research specifically validating this model.
When Should You Choose Exercises Alone vs Devices vs Combination Therapy?
The evidence-based decision framework considers severity, previous training experience, access to physiotherapy, and budget constraints.
Choose traditional exercises alone when:
- You’ve received previous physiotherapy instruction and can correctly identify pelvic floor muscles (verified by professional assessment)
- Incontinence is mild (fewer than 2 episodes weekly) and not significantly impacting quality of life
- Budget constraints limit device purchase and insurance doesn’t cover physiotherapy
- You have high self-motivation and don’t require external accountability systems
- Regular physiotherapist monitoring is available to verify technique and progress
Research shows properly performed PFMT produces excellent outcomes. The limitation is that 30-40% of women cannot perform exercises correctly without guidance, and adherence rates average only 40-50% beyond 4 weeks for unguided programs (PMID 21735442).
Choose biofeedback devices when:
- You’ve never received pelvic floor training and need technique verification
- Previous attempts at self-guided Kegels produced minimal improvement (suggesting technique errors)
- Adherence is challenging and you respond well to app-based tracking and gamification
- Incontinence is mild-to-moderate and not complicated by prolapse or chronic pain
- One-time $149-299 device investment is manageable but ongoing physiotherapy costs are prohibitive
- You prefer home-based training over clinic visits
Meta-analyses show biofeedback augmentation improves outcomes by 15-25% compared to written instructions, primarily by ensuring correct technique and improving adherence through objective tracking (PMID 40066950).
Choose electrical stimulation devices when:
- Pelvic floor muscles are severely weak with barely perceptible voluntary contraction
- Postpartum recovery has left you unable to identify or engage pelvic floor muscles
- Neurological conditions impair motor control
- You need passive strengthening as foundation before transitioning to voluntary exercise
- Budget allows $299 device plus ongoing gel pad costs
Research demonstrates EMS effectiveness comparable to PFMT for stress incontinence, with particular value when voluntary contraction is difficult (PMID 39978852). Optimal protocols combine EMS with progressive transition to voluntary exercise.
Choose combination therapy (device + physiotherapy) when:
- Incontinence is moderate-to-severe (multiple daily episodes)
- Pelvic organ prolapse is present (requires professional monitoring)
- Chronic pelvic pain complicates the presentation
- Previous device-only or exercise-only approaches produced inadequate results
- Insurance covers physiotherapy costs or budget allows both interventions
- You want professional assessment with cost-effective home device maintenance
The supervised-plus-device study found single initial physiotherapy session plus home device training produced outcomes comparable to full supervised therapy at one-third the cost (PMID 37185188).
The research verdict: For straightforward stress incontinence, biofeedback devices achieve 54-58% incontinence reduction comparable to fully supervised therapy while costing $299-329 total versus $700-1,200 for supervised programs (PMID 37185188).
What Are the Research Gaps in Current Device Studies?
While pelvic floor muscle training has robust research support, device comparison studies show notable limitations.
Few head-to-head device trials: Most research compares biofeedback-augmented PFMT to standard exercises rather than comparing specific commercial devices. The Perifit study represents one of few published trials examining a specific consumer product (PMID 38516650). Comparative effectiveness research directly testing Perifit vs Elvie vs Yarlap vs physiotherapy would strengthen evidence-based recommendations.
Limited long-term data: Most trials measure outcomes at 12 weeks or 6 months. Few studies track device users beyond one year to assess sustained benefit, adherence to maintenance training, or durability of improvement. The 5-year PFMT follow-up studies used physiotherapist-supervised programs rather than consumer devices.
Predominantly white study populations: Published trials recruit primarily white European and North American participants. Research including diverse racial and ethnic groups would clarify whether outcomes generalize across populations with different pelvic floor anatomy or cultural attitudes toward internal device use.
Incomplete adherence reporting: Studies measure whether women complete assigned training but rarely track how consistently they use devices beyond trial requirements. Real-world adherence patterns with consumer-purchased devices may differ from research settings with regular study coordinator contact.
App data privacy questions: Commercial biofeedback devices collect detailed health data through smartphone apps. Published research does not address privacy practices, data security, or third-party sharing policies. The biofeedback pelvic floor device guide examines these considerations.
Unclear optimal training protocols: Studies use varied protocols (3-5x weekly, 10-20 minute sessions, 8-12 week duration) making it difficult to identify the minimum effective dose. More granular research could optimize efficiency.
Limited economic analyses: Few studies conduct formal cost-effectiveness analyses comparing devices to physiotherapy or other treatments. The home-device trial provided valuable economic data, but broader health system analyses would inform insurance coverage decisions (PMID 37185188).
Mechanism questions: While research demonstrates biofeedback improves outcomes, the relative contribution of technique verification vs adherence tracking vs gamification engagement remains unclear. Studies dismantling these components could refine device design.
Despite these limitations, the existing evidence base from multiple randomized trials and systematic reviews provides strong support for biofeedback-augmented PFMT compared to unguided exercise, particularly for technique verification and adherence improvement.
Research perspective: Current evidence strongly supports biofeedback device use for stress incontinence, while acknowledging gaps in long-term data, device comparisons, and diverse population studies.
How Can You Integrate Pelvic Floor Training with Other Pelvic Health Strategies?
Pelvic floor strength represents one component of comprehensive pelvic health, interacting with other factors that influence incontinence and organ support.
Hormonal considerations: Declining estrogen during menopause thins vaginal tissue and reduces muscle tone. A 2024 study found women using local vaginal estrogen plus PFMT achieved 25% better outcomes than exercise alone (PMID 39499517). The best perimenopause supplements article examines hormonal support options, while best magnesium for women over 40 discusses mineral support for muscle function.
Core strength integration: Pelvic floor muscles work synergistically with deep abdominal muscles (transverse abdominis) and diaphragm as part of the core cylinder. Research shows women with better core stability achieve superior pelvic floor outcomes. Integration with Pilates or targeted core work may enhance results, though high-impact exercise should be avoided during initial strengthening phases.
Weight management: Excess body weight increases intra-abdominal pressure, stressing pelvic floor muscles. Studies show 5-10% weight loss improves incontinence by approximately 50%, comparable to PFMT effects. Combined approaches produce additive benefits.
Fluid and dietary management: Caffeine, alcohol, carbonated beverages, and acidic foods irritate bladder tissue, worsening urgency symptoms. Behavioral modifications addressing these triggers complement muscle strengthening for mixed incontinence presentations.
Constipation management: Chronic straining weakens pelvic floor muscles over time. Adequate fiber intake (25-30g daily), hydration, and magnesium supplementation support regular bowel movements, reducing downward pressure on pelvic organs.
Breathing pattern optimization: Paradoxical breathing patterns (chest breathing vs diaphragmatic breathing) alter intra-abdominal pressure distribution. Physiotherapists often teach diaphragmatic breathing as part of comprehensive pelvic floor rehabilitation.
Vaginal health: Vaginal dryness or atrophy makes device use uncomfortable. Local vaginal moisturizers or estrogen therapy may be needed before beginning internal device training.
A 2024 conservative treatment overview emphasized multifactorial approaches addressing lifestyle, behavioral, and exercise components typically produce better long-term outcomes than single-modality interventions (PMID 36053030).
Integrative recommendation: View pelvic floor training as one element of comprehensive pelvic health strategy including appropriate hormonal support, weight management, dietary optimization, and breathing pattern awareness.
How Do You Build a Sustainable Training Routine?
Research demonstrates effectiveness under controlled trial conditions, but real-world success requires translating protocols into sustainable daily habits.
Start with professional assessment: Even when planning device-based home training, single physiotherapist evaluation provides valuable baseline information. The assessment verifies you’re strengthening the correct muscles, rules out prolapse requiring different treatment, and identifies whether muscles are weak (requiring strengthening) or overly tight (requiring relaxation training).
Begin conservatively: Initial enthusiasm often leads to over-training and pelvic floor fatigue. Start with 5-minute sessions 3x weekly, gradually increasing to 10 minutes 4-5x weekly as strength improves. Progressive overload drives adaptation, but pelvic floor muscles require 48 hours recovery between intensive sessions just like other skeletal muscles.
Anchor to existing habits: Adherence research shows highest completion rates when new behaviors attach to established routines. Link pelvic floor training to existing habits—morning coffee, bedtime routine, or immediately after brushing teeth. The Perifit app allows customized reminder timing to support habit formation.
Track objectively: Device data provides concrete evidence of improvement that sustains motivation during the slow 8-12 week adaptation period. Review weekly progress charts showing increasing contraction strength or reduced incontinence episodes. Celebrate small wins—25% improvement merits recognition even when not yet achieving full continence.
Combine passive and active methods: For severe weakness, consider starting with 4-6 weeks of EMS training (Yarlap) to build baseline strength, then transitioning to biofeedback device (Perifit) to develop voluntary motor control. The combination study showed this sequencing produced superior outcomes (PMID 36332826).
Plan for plateaus: Strength gains follow non-linear patterns with periods of rapid improvement followed by plateaus. When progress stalls, try varying workout types (endurance vs power vs coordination), increasing resistance, or adding core stability work. Plateaus are normal adaptation phases, not signs of failure.
Transition to maintenance: Once achieving satisfactory symptom control (typically 8-12 weeks), reduce training frequency to 2-3x weekly. Long-term follow-up studies show maintenance training preserves benefits while complete cessation leads to gradual regression over 6-12 months.
Integrate with functional activities: Beyond device workouts, practice engaging pelvic floor before coughing, sneezing, lifting, or jumping—the functional integration that reduces real-world leakage. This “knack” technique reinforces voluntary control during daily stress situations.
Manage expectations realistically: Research shows 50-70% reduction in incontinence episodes, not necessarily 100% cure. Complete continence may require combination with weight loss, dietary modification, or medical treatments. Viewing PFMT as one valuable tool among several sets realistic expectations.
When to seek additional help: If device-guided training for 12 weeks produces minimal improvement (less than 25% symptom reduction), consult a pelvic floor physiotherapist. You may have technique errors the device isn’t catching, pelvic floor tension rather than weakness, or conditions requiring different treatment approaches.
What the data says: Start with minimal viable routine (3x weekly for 5 minutes) and build gradually to 4-5x weekly for 10 minutes. Adherence research shows 70% completion rates with device apps versus 43% with paper logs (PMID 38516650).
When Are Devices Not Appropriate: Contraindications and Cautions
While pelvic floor trainers show excellent safety profiles in published research, certain conditions require medical clearance or alternative approaches.
Absolute contraindications (do not use without medical supervision):
- Active pelvic infection or sexually transmitted infection
- Unexplained vaginal bleeding
- Recent pelvic surgery (typically 6-8 week clearance required)
- Moderate-to-severe pelvic organ prolapse (stage 3-4)
- Pregnancy (most devices not tested for pregnancy safety; consult obstetrician)
- Pacemakers or implanted electrical devices (for EMS devices only)
- Cancer within pelvic region
Relative contraindications (use with caution and professional guidance):
- Mild prolapse (stage 1-2): May benefit from PFMT but requires physiotherapist verification that training isn’t worsening prolapse
- Vaginal atrophy or dryness: Makes device insertion uncomfortable; address with local estrogen or moisturizers before beginning training
- Chronic pelvic pain: May indicate hypertonic (overly tight) muscles requiring relaxation rather than strengthening
- Menstruation: Device use during menstruation is hygienically challenging; most users pause training during heavy flow days
- Latex sensitivity: Ensure devices are medical-grade silicone, not latex
- IUD with strings: Generally safe but consult provider if strings feel displaced after device use
When exercises are preferable to devices:
Research shows biofeedback devices improve outcomes primarily in women who struggle with technique or adherence. For women with good body awareness who can correctly identify pelvic floor muscles and maintain consistent self-directed practice, devices may provide marginal added benefit. The cost difference might be better invested in physiotherapy sessions for personalized instruction rather than home devices.
Psychological considerations: Some women report discomfort with internal device use unrelated to physical sensation. Cultural attitudes, history of sexual trauma, or body image concerns may make traditional exercises preferable. Effective pelvic floor training can occur through exercises alone—devices are enhancement tools, not requirements.
Age considerations: Published research includes women ages 18-80, finding benefits across age ranges. However, postmenopausal women often require longer training duration (12-16 weeks vs 8-12 weeks for premenopausal) and may benefit from concurrent local estrogen therapy to improve tissue quality.
Safety monitoring: Discontinue device use and consult healthcare provider if experiencing:
- Pain during or after use (mild initial discomfort is normal; sharp or persistent pain is not)
- Bleeding after device use
- Worsening incontinence symptoms
- New pelvic pressure or bulging sensation (possible prolapse)
- Urinary retention or difficulty emptying bladder
The comprehensive safety profile from published trials shows adverse events are rare when devices are used appropriately. The Perifit study reported zero serious adverse events among 120 participants over 12 weeks (PMID 38516650).
Safety summary: Pelvic floor devices demonstrate excellent safety when used for appropriate indications after ruling out contraindications. Professional assessment before beginning training ensures device selection matches individual presentation.
What Are the Cost Differences: Devices vs Physiotherapy vs Combined Approaches?
Understanding the full economic picture requires considering not just initial costs but long-term expenses, potential savings from avoided medical treatments, and quality-of-life value.
Device costs:
- Budget biofeedback device (Kegel Exerciser): $107 one-time
- Mid-range biofeedback (Perifit): $149 one-time
- Premium biofeedback (Perifit Care+): $179 one-time
- EMS device (Yarlap): $299 plus $15-20/month consumables
- Replacement/second user: Probe covers $15-20 (devices shareable with hygiene barriers)
Physiotherapy costs:
- Initial assessment: $150-200
- Follow-up sessions: $100-150 each
- Typical 12-week program: 6-8 sessions = $700-1,200
- Insurance coverage: Highly variable (0-80% depending on plan)
Combined approach:
- Single assessment + home device: $150 + $149 = $299
- Produces outcomes comparable to full supervised therapy (PMID 37185188)
- Represents optimal cost-effectiveness for uncomplicated cases
Long-term economic modeling:
Device becomes more cost-effective than ongoing physiotherapy after approximately 3 months. For women requiring maintenance training beyond initial strengthening, devices provide 5-fold cost savings over years 2-5 compared to periodic physiotherapy visits.
However, the calculation shifts when considering insurance coverage. If insurance covers 80% of physiotherapy costs, the out-of-pocket expense ($140-240 for full program) becomes comparable to device purchase, making professional supervision economically attractive.
Avoided medical costs:
Successful incontinence treatment potentially avoids:
- Absorbent pad costs: $15-30/month for daily users = $180-360/year
- Urologist consultations: $200-300 per visit
- Prescription medications (anticholinergics for urgency): $30-60/month
- Surgical procedures (mid-urethral sling): $5,000-15,000
Economic analyses suggest effective conservative treatment (devices or physiotherapy) represents excellent value when avoiding progression to medical or surgical interventions.
Quality-of-life economic value:
Research measuring quality-adjusted life years (QALYs) finds successful incontinence treatment produces QALY gains comparable to many accepted medical interventions. The improved quality of life—reduced anxiety, better sleep, restored social activities, improved sexual function—has substantial value beyond direct cost savings.
A 2024 health economics study concluded biofeedback devices represent “highly cost-effective” interventions under standard thresholds ($50,000 per QALY gained), primarily due to low cost and demonstrated effectiveness in reducing incontinence burden.
Value optimization strategies:
- Start with single physiotherapist assessment ($150-200) to verify diagnosis and rule out contraindications
- Purchase mid-range biofeedback device ($149) for home training
- Schedule follow-up physiotherapist session at 6-8 weeks to verify progress and technique
- Continue device-based maintenance training long-term
This approach combines professional oversight with cost-effective home training, total investment approximately $400-500 versus $700-1,200 for fully supervised therapy.
Economic perspective: For straightforward stress incontinence, biofeedback devices provide excellent value through one-time investment, unlimited use, and outcomes comparable to supervised therapy. Professional assessment remains valuable for diagnosis verification and complex cases.
How Can You Build Exercise Consistency: What Does Adherence Research Show?
The most effective pelvic floor program delivers no benefit if not followed consistently. Adherence research identifies specific strategies that improve long-term compliance.
Implementation intentions: General goals (“I should do Kegels regularly”) show poor adherence. Specific implementation intentions (“I will use my Perifit device for 7 minutes every morning after coffee while checking email”) increase completion rates by 30-40% in behavioral research. Device users should specify exact when, where, and how details.
Habit stacking: Attach new behaviors to existing strong habits. The Perifit app suggests anchoring workouts to established routines—morning bathroom visits, bedtime preparation, or daily meditation practice. Research shows behaviors attached to existing habits achieve 60% higher long-term adherence than standalone new routines.
Temptation bundling: Pair pelvic floor training with enjoyable activities available only during workouts. Reserve favorite podcasts, music playlists, or TV shows for device training time. Studies show this behavioral economics approach substantially improves adherence to unpleasant but beneficial behaviors.
Social accountability: Share goals with partners, friends, or online communities. The Perifit app includes optional sharing features allowing users to compare progress with friends. Research shows public commitment increases goal completion by 30-50% compared to private intentions.
Progress tracking visualization: The human brain responds powerfully to visual progress indicators. Device apps display strength improvement charts, workout streaks, and achievement badges. Behavioral research shows visual progress tracking increases sustained adherence by 40-60% compared to no feedback.
Realistic scheduling: Over-ambitious initial goals lead to failure and discouragement. Start with minimal viable routine (3x weekly for 5 minutes) and build gradually. Research shows sustainable behavior change follows “too easy to fail” principles rather than maximal effort approaches.
Anticipating obstacles: Mental contrasting techniques require identifying likely barriers (travel, busy weeks, illness) and pre-planning solutions. “If I’m traveling, I’ll pack my device and do morning sessions in hotel bathroom.” This if-then planning increases adherence during challenging periods.
Self-compassion over self-criticism: Behavioral research shows self-compassion after missed sessions predicts better long-term adherence than self-criticism. “I missed three days, but I’m back on track today” outperforms “I always fail at sticking with programs.” Device apps that celebrate return after gaps rather than highlighting missed days may improve sustained use.
Periodic re-commitment: Adherence naturally declines over time. Research suggests scheduling monthly “re-commitment moments”—reviewing original goals, celebrating progress, adjusting approach if needed. The 12-week mark often shows adherence decline as initial enthusiasm wanes; explicit re-commitment reduces dropout.
Graduated self-monitoring: Initially intensive tracking (logging every session) helps establish habits. Once routines become automatic (typically 6-8 weeks), reduce monitoring frequency to avoid tracking fatigue. Research shows graduated reduction in self-monitoring maintains behavior better than either constant intensive tracking or early monitoring cessation.
The Perifit adherence rate of 70% at 12 weeks versus 43% for paper-based tracking demonstrates how device features—automated reminders, progress visualization, gamification—operationalize behavioral science principles that improve long-term compliance (PMID 38516650).
Adherence recommendation: Combine device features (reminders, tracking, gamification) with behavioral strategies (habit stacking, temptation bundling, if-then planning) to build sustainable routines that persist beyond initial motivation.
Related Reading
- Best Pelvic Floor Trainer — Evidence-Based Comparison of 2026 Models
- Elvie Trainer Review — Clinical Evidence and Real-World Outcomes
- Kegel Exerciser for Postpartum Recovery — Research-Backed Protocols
- Pelvic Floor Trainer for Menopause — Hormonal Changes and Device Selection
- Biofeedback Pelvic Floor Device — Technology Comparison and Clinical Evidence
- Best Magnesium for Women Over 40 — Perimenopause and Bone Health
- Best Perimenopause Supplements — Evidence-Based Hormone Support
Frequently Asked Questions
Q: Are pelvic floor devices more effective than manual Kegel exercises? Published studies show biofeedback devices produce 15-25% better outcomes for stress incontinence than unguided Kegels, primarily by improving exercise technique and adherence. The OPAL trial (PMID 33289476) found device-guided training reduced incontinence episodes more effectively than basic instruction alone.
Q: How much do pelvic floor trainers cost compared to physiotherapy? Home biofeedback devices range from $107-$299, while physiotherapist-supervised pelvic floor training typically costs $700-$1,200 for a 12-week program. Research suggests home devices with app guidance provide comparable outcomes to supervised training for mild-to-moderate incontinence.
Q: Can electrical stimulation devices replace Kegel exercises? Electrical stimulation (EMS) devices contract muscles passively and work best when combined with active Kegels rather than as a replacement. Studies show combination therapy produces 71% reduction versus 48-52% for either approach alone.
Q: How long does it take to see results from pelvic floor exercises vs devices? Both approaches require 8-12 weeks for measurable improvement. Device users often report earlier progress (4-6 weeks) because biofeedback confirms correct muscle activation, while those doing unguided exercises may spend weeks performing ineffective contractions.
Q: Do I need a device if I can do Kegels correctly on my own? If you can identify and isolate pelvic floor muscles (verified by a physiotherapist), manual exercises may be sufficient. However, research shows 30-40% of women cannot perform Kegels correctly without guidance, making devices valuable for technique verification.
Our Top Recommendations
Best Overall:
Perifit Care+ Pelvic Floor Exerciser
Check Price on AmazonAs an Amazon Associate we earn from qualifying purchases.
Best for Electrical Stimulation:
Yarlap AutoKegel Pelvic Floor Trainer
Check Price on AmazonAs an Amazon Associate we earn from qualifying purchases.
Best Budget:

Perifit Pelvic Floor Exerciser
Check Price on AmazonAs an Amazon Associate we earn from qualifying purchases.
Best Value:

Kegel Exerciser with Probe
Check Price on AmazonAs an Amazon Associate we earn from qualifying purchases.
Join the discussion: Facebook | X | YouTube | Pinterest
Conclusion
The research comparing pelvic floor exercises to training devices reveals that both approaches work effectively, with the key difference lying in technique accuracy and long-term adherence. Traditional Kegel exercises remain the foundation of pelvic floor rehabilitation, supported by decades of randomized controlled trials showing 50-70% improvement in stress incontinence symptoms when performed correctly for 12 weeks.
Biofeedback devices like the Perifit Care+ ($179) bridge the critical gap between knowing what to do and doing it correctly. Published systematic reviews demonstrate 15-25% better outcomes when biofeedback augments standard exercises, primarily because real-time feedback catches the technique errors that affect 30-40% of women attempting unguided training. For women with severe weakness who struggle with voluntary contraction, electrical stimulation devices like the Yarlap ($299) provide passive strengthening as a stepping stone to active exercise.
The most cost-effective approach for most women combines a single physiotherapy assessment ($150-200) with a home biofeedback device ($149-179), producing outcomes comparable to fully supervised programs at one-third the cost. Whether you choose exercises alone, device-assisted training, or combination therapy, consistency remains the strongest predictor of success — and device adherence rates of 70% versus 43% for unguided exercise suggest technology meaningfully supports the sustained effort required for lasting improvement.
References
- Hagen S, et al. Basic versus biofeedback-mediated intensive pelvic floor muscle training for women with urinary incontinence: the OPAL RCT. PMID 33289476
- Dumoulin C, et al. Pelvic floor muscle training with feedback or biofeedback for urinary incontinence in women. PMID 40066950
- Herderschee R, et al. Feedback or biofeedback to augment pelvic floor muscle training for urinary incontinence in women. PMID 21735442
- Kim JK, et al. Effect of personalized extracorporeal biofeedback device for pelvic floor muscle training. PMID 31793032
- Fitz FF, et al. Pressure-mediated biofeedback with pelvic floor muscle training for urinary incontinence. PMID 39499517
- Leitner M, et al. Effectiveness of pelvic floor muscle training alone or combined with other modalities. PMID 36332826
- Kim SH, et al. Pelvic floor muscle training using extracorporeal biofeedback device. PMID 23052631
- Szumilewicz A, et al. Efficacy of supervised pelvic floor muscle training with home-based biofeedback device. PMID 37185188
- Milne JL, et al. Non-surgical management of urinary incontinence. PMID 39978852
- Dumoulin C, et al. Conservative interventions for treating urinary incontinence in women: Overview of Cochrane reviews. PMID 36053030
- Wu Y, et al. Pelvic floor muscle contraction automatic evaluation algorithm. PMID 38575899
- Pelvic floor muscle training using the Perifit device for treatment of urinary incontinence. PMID 38516650
Recommended Products
Get Weekly Research Updates
New studies, updated reviews, and evidence-based health insights delivered to your inbox. Unsubscribe anytime.